The ║┌┴╧│╘╣╧═Ї News Minute is available every Thursday via direct download or the RSS feed.
July 23
Jackie Forti├йr reads this weekтАЩs news: Coverage disruptions can have fatal consequences when switching health plans. Plus, more states are shaming employers that use your tax dollars to cover health costs for their low-income workers.
0:000:00
Speed
July 16
Sam Whitehead reads the weekтАЩs news: Some health plans are pocketing their enrolleesтАЩ drug discounts, while many Affordable Care Act insurers want to raise rates by double digits next year.
0:000:00
Speed
July 9
Rachel Spears reads the weekтАЩs news: When babies receiving infant formula allegedly get sick or die, what happens next is largely up to the companies that make it. Plus, abortions continue to rise four years after the overturning of Roe v. Wade.
0:000:00
Speed
July 2
┤│▓╣│ж░ь╛▒▒Ё&▓╘▓·▓є▒ш;╣ґ┤╟░ї│┘╛▒├й░ї&▓╘▓·▓є▒ш;░┌FOR-tee-ay] reads the weekтАЩs news: More Americans than ever are surviving cancer and face lingering mental health issues. Plus, tips to get your health insurance company to pay for a GLP-1 drug.
0:000:00
Speed
June 25
Zach Dyer [DYE-er] reads the weekтАЩs news: The U.S. is getting its first new sunscreen ingredient in decades. Plus, at-home cancer tests have their limits.
0:000:00
Speed
June 18
Katheryn Houghton [CATH-er-in HOW-tun] reads the weekтАЩs news: New rules that require millions of Americans to work to access Medicaid are stricter than many expected. Plus, the federal Family and Medical Leave Act protects many peopleтАЩs jobs тАФ but thereтАЩs a big catch.
0:000:00
Speed
June 11
Sam Whitehead reads the weekтАЩs news: More Americans are getting access to physician-assisted suicide as states legalize the practice. Plus, hundreds of people allege medical neglect in ICE detention centers.
0:000:00
Speed
June 4
Arielle Zionts [arr-ee-ELL ZY-ence] reads the weekтАЩs news: For some older adults, the risks of certain preventive screenings might outweigh the rewards. Plus, cost spikes for Obamacare plans have consumers seeking cheaper health coverage, which is often less comprehensive.
0:000:00
Speed
May 28
Jackie Forti├йr [FOR-tee-ay] reads this weekтАЩs news: Suicide prevention experts argue that improving AmericansтАЩ financial well-being could save lives. Plus, the Trump administration proposes looser artificial intelligence safeguards to speed innovation in healthcare.
0:000:00
Speed
A Death Revives Concerns About Police Brutality Six Years After National Reckoning
A Death Revives Concerns About Police Brutality Six Years After National Reckoning
Pallbearers carry Lloyd Gilmore to his grave in Sikeston, Missouri. Gilmore died in police custody after an altercation with Sikeston police officers on June 10. (Cara Anthony/║┌┴╧│╘╣╧═Ї News)
A Death Revives Concerns About Police Brutality Six Years After National Reckoning
SIKESTON, Mo. тАФ Not everyone at Lloyd GilmoreтАЩs funeral knew him well. One woman, who had ironed her clothes two days in advance, said she just wanted to be there for his family. School-age children, guided by their parents, approached his open casket in the sanctuary of Cornerstone Baptist Church and peeked inside. Other people looked away.
On that rainy Friday afternoon, hundreds of such mourners gathered to honor the man who went to the police department for help and didnтАЩt come back.
тАЬStay woke. Stay guarded,тАЭ his daughter Lania Gilmore told the church full of mourners in this city of fewer than 16,000 with a long, troubled history of racial violence. тАЬBe there for your family and love on one another.тАЭ
Her father, a 44-year-old Sikeston resident, died in police custody on June 10. During a quick, physical altercation involving seven Sikeston police officers, he was shocked with a Taser and put into hobble restraints, which allow officers to hogtie a personтАЩs feet and hands, according to a through a public records request. Two autopsies were performed, but they тАФ and GilmoreтАЩs cause of death тАФ had not been released as of mid-July while the result of a toxicology report remained pending.
Gilmore had approached an officer in the parking lot of the police station, according to the report, speaking words the officer said he could not understand. Lania Gilmore said that her dad, who had mental health issues, had asked her to call the police department and that he ran there seeking help.
тАЬI kind of trusted the fact that he was OK because he was at the police station,тАЭ she told ║┌┴╧│╘╣╧═Ї News.
Lloyd Gilmore, a 44-year-old Sikeston resident, had been looking for a safe space on the day he died, said his daughter Lania Gilmore. He told her to call the police department for help. Before he died, the police shocked him with a Taser and put him into hobble restraints. (Lania Gilmore)
Some of Lloyd GilmoreтАЩs children embrace during his funeral on June 26 at Cornerstone Baptist Church in Sikeston. тАЬStay woke. Stay guarded,тАЭ his daughter Lania Gilmore (left) told the church full of mourners. тАЬBe there for your family and love on one another.тАЭ (Cara Anthony/║┌┴╧│╘╣╧═Ї News)
A plaque is displayed during Lloyd Gilmore’s funeral. Hundreds of mourners gathered in his honor. (Cara Anthony/║┌┴╧│╘╣╧═Ї News)
At his funeral, hardly anyone spoke of the police тАФ and, at the familyтАЩs request, the funeral home declined to ask police to provide traffic assistance as they usually would. A preacher did his best to comfort GilmoreтАЩs family. тАЬSometimes we need not talk,тАЭ the Rev. Tommy Robinson Jr. told the crowd. тАЬWe just need to listen.тАЭ
But after years of expressing concerns of racial bias within the cityтАЩs police department, some Black Sikeston residents wonder if anyone is listening at all anymore. They want justice even as the national reckoning over police brutality has faded from public view.
тАЬWe need the police. We just need them to do their jobs correctly and leave Black people alone,тАЭ said Mark Wiggins, president of SikestonтАЩs NAACP branch. тАЬThey know it. We know it. The truth of the matter is thereтАЩs a lot of unwarranted cop killings of Black men in America.тАЭ
Mark Wiggins, president of the local NAACP branch, sits outside his Sikeston, Missouri, home. Wiggins grew up in the city, which has a history of racial violence. After Lloyd Gilmore died in police custody on June 10, Wiggins protested alongside other residents and civil rights activists. (Cara Anthony/║┌┴╧│╘╣╧═Ї News)
Email Sign-Up
Subscribe to ║┌┴╧│╘╣╧═Ї News' free Morning Briefing.
But despite worldwide protests in 2020 in the wake of high-profile police-involved killings of Black people, the public paid little attention when a prestigious group released a report last year about deaths in custody, said Roger Mitchell Jr., a forensic pathologist finishing his term as president of the , which represents African American physicians. The urged Congress to require states to collect and report data on all in-custody deaths, a problem that Mitchell said disproportionately affects Black men.
тАЬWe are in an anti-diversity environment,тАЭ Mitchell said. тАЬWeтАЩre in a war.тАЭ
Upon returning to the White House last year, President Donald Trump that targeted diversity, equity, and inclusion programs. As a result of that and other measures, funding for racial equity has dwindled, researchers who once studied violence as a public health issue have redirected their work to less politically charged topics, and a growing fear of professional and political retaliation has made it increasingly difficult to sustain the momentum.
Kevin Myles, a civil rights leader based in Georgia who has trained tens of thousands of activists around the country, said he saw a shift in priorities around racial equity before Trump was reelected. Since then, it has escalated, he said, and he has lost at least half his funding for his work on equity, child welfare, and mass incarceration.
тАЬI donтАЩt think we really were prepared. ItтАЩs not that we didnтАЩt take it seriously. I donтАЩt think we were psychologically prepared for what this means,тАЭ Myles said. тАЬEverything we have done before now was practice. The game has just started.тАЭ
Sikeston, located in the rural area of southeastern Missouri known as the Bootheel, has a history of racial violence, including the brutal lynching of a Black man named Cleo Wright in 1942. Another Black man, Undraus Nabors, was found dead in a grain silo months after heading out to pick up his white girlfriend in 1999. In April 2020, less than a month before George FloydтАЩs murder in Minneapolis, an unarmed Black man, Denzel Taylor, was shot at least 18 times by Sikeston police officers. The city was the subject of the 2024 тАЬSilence in SikestonтАЭ documentary film and podcast by ║┌┴╧│╘╣╧═Ї News, Retro Report, and WORLD.
The тАЬSilence in SikestonтАЭ documentary film explores how the nationтАЩs first federally investigated lynching and a police killing 78 years apart haunt the same rural Missouri community. The film from ║┌┴╧│╘╣╧═Ї News and Retro Report explores the lasting impact of such trauma тАФ and what it means to speak out about it.
Larry McClellon, a longtime Sikeston resident who founded a civil rights group called And Justice for All, has expressed concerns about the integrity of his cityтАЩs police department for decades. HeтАЩs also convinced that being vocal about racism in Sikeston comes with a price.
тАЬItтАЩs a dark side of Sikeston that a lot of people do not know and donтАЩt prefer to know,тАЭ McClellon told ║┌┴╧│╘╣╧═Ї News in 2021 after police fatally shot Denzel Taylor. тАЬBut IтАЩve walked the streets.тАЭ
He believes someone burned down the headquarters of And Justice for All in 2019. A said the fire was тАЬsuspicious in nature.тАЭ The electricity in his building wasnтАЩt on when flames erupted, he said, so he wasnтАЩt satisfied when an investigator called it an electrical fire. He asked the department to take another look. No one was charged.
The headquarters of And Justice for All, a civil rights advocacy group in Sikeston, was destroyed in a 2019 fire. A report from the cityтАЩs public safety department says the 2019 fire was тАЬsuspicious in nature.тАЭ Larry McClellon, a longtime Sikeston resident who founded the group, has expressed concerns about racial violence in the community. (Cara Anthony/║┌┴╧│╘╣╧═Ї News)
James McMillen, the cityтАЩs police chief, told ║┌┴╧│╘╣╧═Ї News in 2021 that he had plans to improve policing before Taylor died. At the time, McMillen, who is white, said he and his department had тАЬa poor relationshipтАЭ with Black residents in the city. He started some community meetings after TaylorтАЩs death, but he said in 2024 that people had stopped showing up.
тАЬWe have tried,тАЭ the chief said during a this month. тАЬBut, as my daddy would say, a relationship is a two-way street. And so I donтАЩt know what else I can do.тАЭ
During the meeting, Lania Gilmore pleaded with the city to release more information about her fatherтАЩs case. Other residents wanted to know why the officers involved were not placed on administrative leave immediately after Gilmore died.
тАЬIt depends on the circumstances. It does,тАЭ McMillen told them. тАЬYouтАЩre assuming a certain set of details that you donтАЩt know.тАЭ
Another resident asked the city about training for officers. McMillen said his officers are trained. Nationwide, many communities have to assist people in crisis.
тАЬChief does not want anybody to be mistreated at all. Period,тАЭ Sikeston Mayor Greg Turnbow, who is white, said at the meeting. тАЬAnd I guarantee you, I put my life in his hands. IтАЩd do it today.тАЭ
McMillen declined to comment on ║┌┴╧│╘╣╧═Ї NewsтАЩ questions about GilmoreтАЩs case and the communityтАЩs concerns about the department. The Missouri State Highway Patrol investigated the death and planned to refer the results to the Cape Girardeau County prosecuting attorney, Sgt. Bradley Germann said.
Lloyd GilmoreтАЩs friends Tawanna and Willie Wilson wore custom T-shirts to his funeral. (Cara Anthony/║┌┴╧│╘╣╧═Ї News)
Andre Young and his 5-year-old son view GilmoreтАЩs body during the funeral. (Cara Anthony/║┌┴╧│╘╣╧═Ї News)
Cynthia Gilmore sits in the front row of her sonтАЩs funeral at Cornerstone Baptist Church. (Cara Anthony/║┌┴╧│╘╣╧═Ї News)
The day Gilmore died, his daughter said, he had been anxious and was looking for a тАЬsafe space.тАЭ So, she said, he had spent much of the day watching her braid hair at the salon where she works, then he went with her to her eyelash extension appointment. Lania Gilmore said he was still feeling undone, but she needed some space, so he asked her to call the police instead. She said she did, then she watched him run toward the police station.
The rest unfolded within 30 minutes, according to the police report and . The police report said that, amid an ensuing scuffle, Gilmore bit one officerтАЩs hand тАФ тАЬbut did not break the skin.тАЭ
After the police stunned and restrained Gilmore, a paramedic gave him a sedative, and the emergency medical services took him to a hospital, according to the police report. The report listed five victims тАФ all police тАФ and accused Gilmore of third-degree assault and resisting arrest.
Lania Gilmore said police told her that her father overdosed. But she said she doesnтАЩt understand how that would have been possible, given the short time between when he left her and an ambulance was called.
The cityтАЩs police force knew Gilmore had mental health issues, his daughter said. Police officers in a neighboring community тАЬexcessively tasedтАЭ and beat him in 2020, . He received a $65,000 settlement five years later, and she said that experience left a mark.
After Gilmore died, Louis Houston, a longtime Sikeston resident, said he decided to move 30 minutes outside the city to a neighboring community, where he feels safer. He said hearing about other Black Sikeston residents being harassed by the police department had started to affect his mental health.
тАЬI got on away from here,тАЭ said Houston, who returned to Sikeston for the funeral.
Louis Houston moved to Sikeston almost 20 years ago but recently decided to move away after Lloyd Gilmore died in police custody. He says the way the police department treats Black residents was affecting his mental health. (Cara Anthony/║┌┴╧│╘╣╧═Ї News)
HoustonтАЩs already thinking about the conversations he will have with his young children about how to respond if they ever interact with a police officer. He has a script in mind.
тАЬBe careful,тАЭ Houston plans to tell them. тАЬThey can help you, but they also can kill you.тАЭ
Every family has secrets. I spent the past few years reporting about racial violence in Sikeston, Missouri. Interviewing Black families there helped me uncover my familyтАЩs traumatic past, too.
Public Health Improvements Stall Amid TrumpтАЩs DEI Crackdown
POSTCARD FROM GEORGIA
Public Health Improvements Stall Amid TrumpтАЩs DEI Crackdown
80 communities across the country saw funding stripped as priorities shifted in Donald TrumpтАЩs second presidency.
Earl Williams, former community development director with the Thomasville Community Development Corp., stands in front of a building the Georgia city hoped would be turned into a healthcare clinic in the Dewey City neighborhood. (Briah Lumpkins/║┌┴╧│╘╣╧═Ї News)
POSTCARD FROM GEORGIA
Public Health Improvements Stall Amid TrumpтАЩs DEI Crackdown
80 communities across the country saw funding stripped as priorities shifted in Donald TrumpтАЩs second presidency.
THOMASVILLE, Ga. тАФ As Earl Williams drove through a historic Black neighborhood known as Dewey City in his hometown, he hardly recognized what he saw.
Homes that once belonged to friends, family, and neighbors had siding covered in mold. Some were boarded up. Others had holes in their roofs.
Black churches once used Oquina Creek, which runs along the border of the neighborhood, to baptize their congregants. Today, fecal bacteria and other contaminants have made the water unsafe due to an aging wastewater system.
тАЬSometimes you get the feeling like youтАЩre in a Third World country,тАЭ Williams said. After three decades in Washington, D.C., he returned four years ago with a mission to revitalize communities such as Dewey City, which he said are тАЬpart of what makes Thomasville, Thomasville.тАЭ
A $19.8 million Community Change Grant from the Environmental Protection Agency was supposed to shift the tides of the neighborhood Williams grew up in.
The city and the , where Williams formerly served as community development director, applied for the grant in 2024. It was part of a $2 billion effort to help disadvantaged communities address environmental health risks and create clean energy and climate resiliency projects.
But three months after winning the grant, Thomasville became one of across the country тАФ from to to тАФ to see the funding stripped as priorities shifted in Donald TrumpтАЩs second presidency.
Black churches once baptized their congregants in Oquina Creek in Thomasville, Georgia. Today, fecal bacteria and other contaminants make the water unsafe. (Briah Lumpkins/║┌┴╧│╘╣╧═Ї News)
Dilapidated houses are common in Dewey City, a historic Black neighborhood in Thomasville. Many residents donтАЩt have the funds to mitigate issues with mold, asbestos, or lead paint. (Briah Lumpkins/║┌┴╧│╘╣╧═Ї News)
On the first day of his second term, Trump signed an executive order titled тАЬ.тАЭ It stated that the Biden administration тАЬforced illegal and immoral discriminationтАЭ through diversity, equity, and inclusion programs.
In an emailed statement, EPA spokesperson Mike Bastasch said the administration is тАЬfully committed to being a great steward of taxpayer dollars.тАЭ He added that the тАЬradical agendaтАЭ of DEI and environmental justice тАЬpreferencingтАЭ are not within the agencyтАЩs core mission of protecting human health and the environment.
Environmental health advocates argue, though, that the decision to cut the grants was not rooted in science. They say that equating environmental justice to DEI is an act of bad faith and that withholding the money forces disenfranchised communities to delay long-overdue updates needed to protect public health for marginalized populations.
тАЬI unfortunately believe weтАЩre going to see a reversal in the health profile of this country,тАЭ said , an associate professor at the University of Michigan who served in the Biden administration as the first federal chief environmental justice officer.
тАЬThis current federal regime has decided that humanity and public health and justice don’t mean anything,тАЭ she said.
Email Sign-Up
Subscribe to ║┌┴╧│╘╣╧═Ї News' free Morning Briefing.
тАШWhy Us?тАЩ
Thomasville, near GeorgiaтАЩs southwestern border, is home to just over 18,600 people.
The city had hoped to improve health outcomes in neighborhoods on its southern and western sides where, according to the grant proposal, тАЬhistorical redlining created a legacy of disinvestment.тАЭ
Those areas have a deep history: Dewey City, for example, was the first neighborhood in the city where Blacks could build homes after the Civil War. ItтАЩs also home to the closed Douglass High School тАФ the first public school for Blacks in Thomasville, established in 1902.
тАЬThis place has been neglected,тАЭ said Williams, who occasionally hosts historical walks through the community. тАЬBut itтАЩs worth bringing it back online.тАЭ
The proposed тАЬRestoring ResiliencyтАЭ project featured a plan to remove toxic substances such as mold, lead paint, and asbestos from homes, repair a nearly 82-year-old wastewater system, and convert part of a shuttered high school band room into a health clinic.
Williams points at the former Douglass High School campus, where a healthcare clinic and тАЬresilience hubтАЭ was planned. (Briah Lumpkins/║┌┴╧│╘╣╧═Ї News)
In a community of mostly older residents who rely on public transportation, a healthcare clinic planned for this building would have increased access to care and built trust, local advocates say. (Briah Lumpkins/║┌┴╧│╘╣╧═Ї News)
тАЬThis was a long and storied attempt to bend the arc of justice closer,тАЭ said Jeremy Rich, a Thomas County commissioner and the pastor at First Missionary Baptist Church. тАЬJustice in healthcare. Justice in environmental impact.тАЭ
Having a clinic in the community would be a тАЬgame changer,тАЭ Rich said. During the covid pandemic, he said, older residents who rely on public transit were reluctant to go to the nearby hospital or the county health department to get vaccinated. When his church offered shots from Black nurses, he said, vaccination rates improved.
The Rev. Jeremy Rich, a pastor, teacher, and Thomas County commissioner, says a clinic in the Dewey City neighborhood of Thomasville would have increased trust in healthcare providers. (Briah Lumpkins/║┌┴╧│╘╣╧═Ї News)
Many residents donтАЩt have the financial means to remove mold, lead paint, and other toxic materials, said Thomasville Mayor Pro Tem Lucinda Brown. тАЬThey just have money to live with every day. ThatтАЩs it,тАЭ she said. тАЬIf they can make that happen.тАЭ
The grant meant hope, and its reversal left many asking, тАЬWhy us?тАЭ Williams said.
In the EPAтАЩs May 2025 letter announcing the grant termination, it said ThomasvilleтАЩs project promoted тАЬinitiatives that conflict with the AgencyтАЩs policy of prioritizing merit, fairness, and excellence.тАЭ The grant was тАЬinconsistent with, and no longer effectuates, Agency priorities,тАЭ the letter said.
Environmental justice projects are rooted in science, not DEI, said Jillian Blanchard, the senior vice president of climate change and environmental justice at , a national nonprofit that provides pro bono legal assistance in focus areas such as health equity, immigration, and environmental health.
тАЬWhere is the water dirty? Where is the air unclean?тАЭ she said. тАЬThat is where the money should go.тАЭ
In June of last year, nearly two dozen communities and organizations around the country filed a to get the Community Change Grants reinstated. The lawsuit argued that the projects тАФ such as efforts to create energy-efficient housing in Kalamazoo, Michigan, and empower Houston residents in the pollution permitting process тАФ were vital.
The case was dismissed by a federal district judge in 2025 but is being appealed.
Thomasville was not named in that lawsuit. But the city did appeal the EPAтАЩs decision on its project with the support of BlanchardтАЩs group. The city and the EPA continue to dispute the issue.
This March, the EPAтАЩs deputy inspector general, which serves as an independent watchdog for the agency, concluding that the process for determining the awardees was fair.
Such federal funding is needed because large-scale change is difficult for small municipalities to achieve without getting stuck with high-interest loans, Blanchard said.
тАЬItтАЩs next to impossible,тАЭ she said. тАЬThatтАЩs one of the reasons the things havenтАЩt been done.тАЭ
Thomasville received nearly $20 million in federal money for improvement in areas like Dewey City. But months later, the Trump administration pulled the funds, citing shifting priorities. (Briah Lumpkins/║┌┴╧│╘╣╧═Ї News)
тАШItтАЩs Not OverтАЩ
The city of Thomasville has found other ways to make some improvements in the meantime. With the help of a nearly $3 million federal Community Development Block Grant from the Department of Housing and Urban Development, it made repairs to portions of Dewey CityтАЩs sewer, water, and drainage systems.
The Thomasville Community Development Corp. has begun building affordable housing in Dewey City and intends to convert a portion of the closed Douglass school into apartments for seniors.
The corporation has also applied for $764,000 in through the office of Sen. Jon Ossoff (D-Ga.) that it hopes to use to construct a community health clinic in Dewey City. Decisions on these funding requests will be made this fall.
тАЬItтАЩs not over,тАЭ said Williams, whose legacy in Thomasville runs deep. At the center of what locals call The Bottom тАФ a two-block stretch of downtown where independent Black and other minority-owned businesses once thrived тАФ is a plaque honoring his father, Earl Williams Jr., the cityтАЩs first Black mayor.
As he peered at his fatherтАЩs memorial on a muggy afternoon, he reaffirmed his intentions.
тАЬThereтАЩs more work to be done, and IтАЩm able,тАЭ he said. тАЬI like pouring into the community.тАЭ
But he has little hope the initial grant will be restored under the current administration.
тАЬThat was our shot. We didnтАЩt do anything to miss it,тАЭ he said. тАЬWe just did it during the wrong period of time.тАЭ
Williams came back to Thomasville after years away, in part to continue a legacy started by his father, Earl Williams Jr., who was ThomasvilleтАЩs first Black mayor and first Black council member. (Briah Lumpkins/║┌┴╧│╘╣╧═Ї News)
American Scientists See Prosecutions as Part of Federal Campaign Against Them
American Scientists See Prosecutions as Part of Federal Campaign Against Them
The National Institutes of HealthтАЩs Rocky Mountain Laboratories in Hamilton, Montana. (Katheryn Houghton/║┌┴╧│╘╣╧═Ї News)
HAMILTON, Mont. тАФ The Trump administration has stepped up arrests and public condemnation of federal scientists studying viruses as the world faces one of its worst Ebola epidemics.
In June, Vincent Munster, an infectious disease researcher at the National Institutes of Health, was charged with bringing biological specimens into the U.S. without proper documents. Weeks later, Sen. Rand Paul (R-Ky.) ordered Anthony Fauci, MunsterтАЩs former boss, to appear before a Senate committee, alleging that heтАЩd lied to Congress about the covid-19 pandemicтАЩs origins. This spring, the FBI detained a former aide to Fauci, and federal officials banned a virus researcher in North Carolina from receiving federal funding.
In each case, senior U.S. officials and members of Congress have leaned into unproven theories that arrogant scientists damaged rather than protected public health by recklessly experimenting with covid and other killer viruses, including in China.
Conservative groups and social influencers have amplified that view through a whirlwind of covid conspiracy theories, bioterrorism fearmongering, and anti-immigration sentiment. The recent charges stirred long-held mistrust of the high-security Rocky Mountain Laboratories, where Munster works, among residents of this blue-collar mountain town in Montana built on logging.
Email Sign-Up
Subscribe to ║┌┴╧│╘╣╧═Ї News' free Morning Briefing.
A dozen scientists interviewed for this article said that any crimes or errors committed by Munster, who was transporting vials of inactivated mpox for research purposes, seemed to be over paperwork and posed no threat to the public. Nonetheless, some colleagues in Montana said, the alleged improprieties needlessly bat a hornetтАЩs nest.
тАЬThis just gives ammunition to the people that are trying to stop this valuable research,тАЭ said Kim Hasenkrug, a scientist emeritus at the NIH who worked at Rocky Mountain Labs for 31 years. тАЬEven people who have trusted us in the past, this sows seeds of distrust. How could it not?тАЭ
Cuts to U.S. foreign aid and research funding have left tens of millions of dollars in gaps in the fight against spreading Ebola and mpox outbreaks, scientists told ║┌┴╧│╘╣╧═Ї News. тАЬWhen the next pandemic comes around and we need vaccines to protect ourselves, the chances are that China will develop them before we do,тАЭ said Kristian Andersen, an evolutionary biologist at Scripps Research. Andersen co-authored studies that stoked the ire of proponents of the theory that a lab leak started the covid pandemic.
Emily Hilliard, a spokesperson for the Department of Health and Human Services, which includes the NIH, said the federal government тАЬremains fully equipped to protect Americans and respond to emerging public health threats.тАЭ She said the Centers for Disease Control and Prevention had deployed experts domestically and internationally to respond to Ebola.
Scientists like Munster are indispensable for figuring out the source of pandemic viruses, whether bats, pigs, rats, or some other animal, Andersen said. Munster тАЬis the person who goes out to Africa to get samples of bad viruses from people,тАЭ said Stanley Perlman, a virologist at the University of Iowa and a longtime member of the FDAтАЩs vaccine advisory panel. тАЬHeтАЩs done lots of things that needed to be done, and he does them well.тАЭ
Authorities arrested Munster and Claude Kwe, a research fellow at Rocky Mountain Labs, June 2 on charges of conspiracy to smuggle mpox into the United States and lying to border agents. They had been stopped Jan. 25 at the Detroit airport after returning from the Republic of Congo.
Vincent Munster (National Institutes of Health)
The announcing the charges said FBI testing had confirmed the viruses were inactivated тАФ Munster helped тАФ but that the scientists jeopardized AmericansтАЩ safety.
тАЬThese NIH experts apparently broke our laws by smuggling viral pathogens on a packed commercial airplane from an outbreak in the Republic of Congo. Let that sink in,тАЭ said Jerome Gorgon, U.S. attorney for the Eastern District of Michigan.
The says Munster and Kwe falsely told customs agents the mpox specimens they brought back were for diagnostic use. Yet several scientists told ║┌┴╧│╘╣╧═Ї News that the specimens most likely were indeed for use in developing mpox diagnostic tests.
The complaint also states that the scientists lacked the appropriate documents. requires researchers to register and certify inactivated viruses.
тАЬHe is presumed innocent and we will have to await future proceedings before commenting,тАЭ KweтАЩs federal community defender, Benton Martin, said of his client.
In Montana, Marshall Bloom, an associate director at Rocky Mountain Labs, told the Ravalli County Board of Health in a July meeting that the scientists have been suspended and arenтАЩt allowed on campus amid an internal NIH investigation. тАЬThese are not trivial accusations,тАЭ Bloom said.
It is not illegal or unheard of to take an inactivated virus on a plane. If the samples were inactive, тАЬthe risk is zero,тАЭ said Daniel Jernigan, who worked for 26 years at the CDC and led its National Center for Emerging and Zoonotic Infectious Diseases until retiring last August.
тАЬBut you have to have the documentation available,тАЭ he added.
Jernigan recalled reprimands issued for this sort of lapse but knew of no arrests.
тАЬIn this climate,тАЭ Perlman said, тАЬyouтАЩd want to make sure you talk to people at your institution to make sure any iтАЩs are dotted and tтАЩs are crossed.тАЭ
MunsterтАЩs attorney didnтАЩt respond to multiple interview requests.
Skeptical Neighbors
Conservative politicians and others skeptical of the nationтАЩs covid response have had Munster and Rocky Mountain Labs on their radar for years.
The facility is in Hamilton, a town of 5,000 in rural Ravalli County, which gave President Donald Trump 69% of its vote in 2024. The lab got its start with studies of Rocky Mountain spotted fever in the 1900s, when ranchers and cattle were dying from the then-unknown disease.
Today it is a Biosafety Level 4 facility, one of only several dozen labs in the world to employ the highest level of safety controls that enable scientists to study the deadliest pathogens.
Munster and his laboratory of viral ecology are known as the тАЬgo-to group for highly dangerous virusesтАЭ such as Middle East respiratory syndrome, Nipah, Ebola, and bird flu, said zoologist Peter Daszak, whose work has also been targeted in recent years. Munster тАЬgoes into red zones,тАЭ gets samples from sick people, and makes diagnostic tests that help assess an outbreak and how to stop it, Daszak said.
Munster and his colleagues contributed to studies of , , and тАФ work that put the lab in the crosshairs of people warning about the dangers of biomedical research.
In April, the White Coat Waste Project, a self-described government watchdog group to stop tax-funded animal testing, paid for billboards across seven cities with NIH-funded labs, including Hamilton.
The next month, about the investigation into Munster, citing an anonymous letter. That caught the attention of Laura Loomer, a far-right activist known as a loyalty enforcer for Trump who has the presidentтАЩs ear. She posted about it to her 1.9 million followers on the social platform X.
тАЬFauci Holdovers at @NIH and @HHSGov are about to unleash Ebola in America,тАЭ Loomer posted on May 17, asking why Munster, who is Dutch, and Kwe, from Cameroon, werenтАЩt imprisoned or deported.
Little more than a week later, Montana Republican U.S. Sen. Tim Sheehy sent a letter to HHS calling for an investigation, saying the alleged improper behavior by the scientists could threaten national security.
Munster and Kwe were charged days later. U.S. Rep. Paul Gosar, an Arizona Republican, in mid-July as a reason to close the Hamilton facility, part of his ongoing тАЬFauci-era programs.тАЭ
The arrests added to local apprehensions about the facility.
тАКтАЬYou can’t pick and choose which rules you follow when you’re dealing with this stuff,тАЭ County Commissioner Jeff Burrows said at a June meeting. тАЬAnd I know he’s innocent until proven guilty, but for GodтАЩs sakes, this is a big deal.тАЭ
The Ongoing Push To Blame Fauci
About two weeks after the charges, departing Director of National Intelligence Tulsi Gabbard released declassified documents that she said proved Fauci had lied to Congress about NIH-funded research at the Wuhan Institute of Virology, the lab that, in her words, тАЬsparked covid.тАЭ The documents, however, provide no new evidence that the lab launched the covid virus. Most, though not all, virus experts think the best evidence indicates the virus jumped from bats to other animals, and then to humans at a Wuhan market.
of the lab-leak theory have issued fresh calls to punish Fauci, 85, and scientists his institute funded. Fauci declined to comment for this article.
Shortly after GabbardтАЩs report, Paul, who chairs the Senate Homeland Security and Governmental Affairs Committee, subpoenaed Fauci to testify before the committee.
Fauci тАЬwas Dr. Frankenstein of the modern eraтАЭ and тАЬhas the blood of millions of people on his hands,тАЭ Peter Navarro, a senior adviser to Trump, on June 25. тАЬYou idiot! … You need to come clean, Fauci.тАЭ
The administrationтАЩs mistrust of the federal bureaucracy and the scientific work it has funded has led to broad cuts and staffing losses, including in .
A May 2025 suspended research on many risky viruses, and HHS later halted an $82 million, that funded research into emerging viruses by 10 labs across the world. In late May this year, the White House that would give political appointees sweeping power over all federally funded science.
Prominent covid experts and scientists close to Fauci have been called before congressional committees, barred from receiving government grants, or arrested.
Marshall Bloom, an associate director at Rocky Mountain Laboratories, provides an update to the Ravalli County Board of Health in July in Hamilton, Montana. Local apprehensions about the National Institutes of Health facility intensified following the recent arrest of two of its scientists for allegedly bringing biological specimens into the U.S. without proper documents. (Katheryn Houghton/║┌┴╧│╘╣╧═Ї News)
In April, heavily armed FBI agents of David Morens, FauciтАЩs 78-year-old former aide. They forced him to strip to his underwear and drove him in handcuffs 40 miles to a federal courthouse, where he was briefly jailed, according to Science magazine. MorensтАЩ case is pending.
In May, HHS told Ralph Baric, a University of North Carolina coronavirus expert, that it was halting his federal funding because of a тАЬpattern of deceptionтАЭ in his communications with the NIH. .
In some ways, the arrests of Munster and Kwe felt unsurprising, said Philip Stewart, a recently retired Rocky Mountain Labs researcher focused on tick-borne diseases.
тАЬThere is an anti-science movement,тАЭ Stewart said. тАЬWe are targets, and if it hadnтАЩt been Vincent, it would have been someone else.тАЭ
Most Americans believe in the lab-leak theory, according to surveys, and several U.S. intelligence agencies lean in that direction. That makes targeting scientists who do that kind of work politically expedient, said Daszak, whose NIH-funded nonprofit worked with Chinese virologists in Wuhan and has been under scrutiny since April 2020, when Trump his funding ended.
Animal viruses jump to humans in the wild a year, usually producing negligible infections, occasionally sparking an outbreak. The Ebola virus causing the current African epidemic may have originated in bats, which seem to carry it without getting sick.
тАЬWhile we sit around removing pandemic preparedness grants, arresting scientists, locking them up in some cases,тАЭ Daszak said, тАЬviruses are out there evolving.тАЭ
TrumpтАЩs Personnel Agency Says It Will Remove Some Identifying Info as It Sweeps Up Medical Records
The Trump administration is forging ahead with a controversial plan to collect the medical records of millions of federal workers and retirees, as well as their family members.
The Office of Personnel Management posted last month that it will begin routinely collecting identifiable, personal health information on more than 8 million people тАФ despite concerns from privacy advocates and Democrats, who have demanded the agency drop the plan. The notice will go into effect July 24, allowing OPM to begin its collection at any point afterward.
In reaction to privacy concerns raised by insurers and others, OPM now says the identities of enrollees will be тАЬpseudonymizedтАЭ тАФ meaning names, addresses, and Social Security numbers will be removed тАФ before the agencyтАЩs analysts review the massive new health datasets it will soon begin receiving.
Birth years of enrollees will be retained, and the agencyтАЩs тАЬtechnical staffтАЭ will receive member IDs that it will scramble into different, unique numbers before releasing them to other staffers, according to the notice.
But the notice also specifies that OPM retains the right to reidentify the records.
Sixty-five insurance companies will be required to routinely send OPM detailed data тАФ including names, addresses, doctor information, diagnoses, prescriptions filled, and payment details тАФ on health care services paid through the Federal Employees Health Benefits and Postal Service Health Benefits programs.
In a change to its original proposal, first reported by ║┌┴╧│╘╣╧═Ї News, the agency says it also wants to peek at records kept by Medicare, the federally funded health insurance for older and disabled Americans, to examine claims from federal employees and retirees, and their families, who depend on both programs.
Email Sign-Up
Subscribe to ║┌┴╧│╘╣╧═Ї News' free weekly newsletter, "The Week in Brief."
In its latest notice, OPM argues that the vast trove of data is necessary to ferret out fraud and overpayments in the FEHB and PSHB programs. Those programs cost roughly , with about $50 billion covered by the federal government and $30 billion funded by enrollees. The Trump administration has ramped up efforts, led by Vice President JD Vance, to curtail what it says is rampant fraud and misuse of publicly funded health benefits.
The effort still faces criticism that it doesnтАЩt go far enough to protect the privacy of federal workers and their families.
тАЬClearly, this administration has not earned our trust with AmericansтАЩ sensitive data,тАЭ Sen. Mark Warner (D-Va.) said in an emailed statement to ║┌┴╧│╘╣╧═Ї News. тАЬIf OPM wants to work in good faith to reduce fraud, they should come to Congress, including to folks like me who are engaged on this issue and represent many federal workers and retirees and their families, and work to build consensus and trust before implementing these sweeping changes.тАЭ
The , posted in December, sparked concerns in part because it did not specify what the Trump administration planned to do with the sensitive health information it receives тАФ and did not instruct insurers to redact identifying information.
OPM General Counsel Kurt Dykstra said the detailed records are critical to the administrationтАЩs mission of rooting out fraud and could help identify fraud perpetrated not only by medical providers but also by enrollees.
But when pressed for instances of workers, retirees, or their relatives committing such fraud, Dykstra only noted generally that healthcare fraud does occur.
The information could demonstrate тАЬpotential anomalies in usage patterns that could be related to the individual, but really also could be related to the provider, the treater, the clinic тАФ whoever it is thatтАЩs actually providing the care,тАЭ Dykstra told ║┌┴╧│╘╣╧═Ї News in an interview.
Records deemed suspicious by OPMтАЩs data analysts could then be referred to the agencyтАЩs Office of the Inspector General for further investigation, which could include тАЬdetermining whoтАЩs involved and what the potential issues are, what the ramifications look like,тАЭ Dykstra said.
OPMтАЩs plan to collect and analyze medical records has prompted unease among unions and federal workers, to mass firings and layoffs тАФ in some cases, they say, driven by political retribution тАФ since President Donald Trump took office.
Health privacy lawyers say, too, that while pseudonymizing workersтАЩ details is a step in the right direction, it might not go far enough to protect their privacy.
OPMтАЩs notice mostly complies with the Health Insurance Portability and Accountability Act, the federal law commonly called HIPAA that protects sensitive health data from being shared, said Matt Fisher, a health privacy lawyer. But he noted one exception: The member ID that insurers provide enrollees can be used to identify them.
тАЬThe described process arguably comes down to trusting internal controls in OPM to ensure that data is walled off as proposed,тАЭ Fisher said in an email. тАЬThe ideal would be for only truly de-identified information to be shared in the first place.тАЭ
Insurers regularly share information about claims with employers who offer health plans to employees, in efforts to control costs. But since employers themselves are not covered by HIPAA, large datasets are typically de-identified, meaning the insurers remove identifying information such as employeesтАЩ names or addresses, to comply with the law.
Employers, too, have been accused of using health information to target employees for dismissals. Most recently, a group of Meta employees filed a lawsuit of using artificial intelligence to target for layoffs those who had taken medical or family leave.
Pseudonymizing details such as names or addresses would go only so far to protect privacy, since medical conditions in particular can make it very easy to identify certain employees, said Joseph Lorenzo Hall, a technologist at the Center for Democracy & Technology, a nonprofit that advocates for data privacy.
тАЬThe richer the data, the more likely it is going to be identifying,тАЭ Hall said.
тАЬIn this case, you may be the only person in a region that has that particular kind of medical procedure, condition, or even prescription,тАЭ he said. тАЬAll of those things can be extremely identifying, even when you remove or obfuscate or pseudonymize direct identifiers.тАЭ
Most federal retirees decide to continue with FEHB plans and enroll in Medicare once they turn 65, which provides more comprehensive coverage and allows family members to remain enrolled in FEHB plans, said John Hatton, the staff vice president for policy and programs at the National Active and Retired Federal Employees Association.
OPM wants to analyze medical records for those dual enrollees as well. The agency is asking for all of their cost and service use records from the Centers for Medicare & Medicaid Services.
Still, Hatton said, OPMтАЩs latest notice provides more details about how the agency says it will use the sensitive health information it receives and safeguard it.
тАЬItтАЩs a big improvement over the last notice, which was very lacking in detail and explanation for why they wanted all the medical claims data and how theyтАЩre going to protect the privacy of the data,тАЭ Hatton said.
тАЬWeтАЩd be open to seeing even more security around the privacy of the data so there really is a clear wall,тАЭ he added.
Severely Ill Prisoners Granted Early Release Are Left Stuck Behind Bars
Severely Ill Prisoners Granted Early Release Are Left Stuck Behind Bars
The Halawa Correctional Facility in Honolulu is ▒с▓╣╖╔▓╣╛▒тАШiтАЩs only medium-security state prison. Its infirmary has six cells where prisoners granted compassionate release often remain until they are able to get placed at a long-term care facility. (Ashley Mizuo/║┌┴╧│╘╣╧═Ї News)
╩╗AIEA, ▒с▓╣╖╔▓╣╛▒тАШi тАФ Christian Alameda used a cane to push himself up out of bed in his cell at the Halawa Correctional Facility in Honolulu. He has been recovering in the prisonтАЩs medical infirmary since a January stroke left the right side of his body mostly paralyzed.
In February, ▒с▓╣╖╔▓╣╛▒тАШiтАЩs parole board granted the now-52-year-old compassionate release, which allows prisoners to receive early probation to seek .
But without a long-term care facility willing to accept him, Alameda has not been able to leave.
As of June, at least three other prisoners granted release to tend to their medical needs were living indefinitely in the infirmary after long-term care facilities were unwilling to accept them, primarily because of their criminal backgrounds, the state parole authority said.
тАЬThis is a challenge across the country,тАЭ said Molly Crane, an attorney for FAMM, which advocates for .
Every state allows for prisoners, though Hawai╩╗i is the only one without a specific law, relying instead on an internal policy. The prisoners who typically qualify for compassionate release canтАЩt care for themselves or have terminal illnesses and may need an assisted living center, a nursing home, or hospice.
But many long-term care facilities nationwide decline to take such prisoners, leaving them incarcerated for months тАФ or years тАФ after they were granted release.
In , a study found that rejections from nursing homes soared after they were told that a patient was coming from prison. , prisoners with extensive medical needs stayed an average of 200 days after being granted parole, because of denials from long-term care centers. And in , prisoners granted parole sued the state when they couldnтАЩt get placed in nursing homes.
President Donald TrumpтАЩs signature One Big Beautiful Bill Act further strains long-term care providersтАЩ ability to take people from incarceration. Prisoners donтАЩt qualify for Medicaid, so parolees after theyтАЩre granted the release. The law, enacted last summer, reduces the window in which facilities can get reimbursed from three months to before they apply. That means facilities risk not getting paid for new Medicaid patients whose applications are not submitted within the reduced timeframe.
The Centers for Medicare & Medicaid Services тАЬencourages providers and beneficiaries to prioritize timely application submission to maximize coverage,тАЭ CMS spokesperson Timothy Foster said.
Email Sign-Up
Subscribe to ║┌┴╧│╘╣╧═Ї News' free weekly newsletter, "The Week in Brief."
тАШRisk Is Just Too HighтАЩ
Most nursing homes nationwide already have a waiting list for new residents, according to a by the American Health Care Association and the National Center for Assisted Living. Those waitlists are another hurdle to getting prisoners placed, said Bob Merce, a former attorney who advocates for prisonersтАЩ compassionate release.
тАЬWe tell the nursing homes that most of the people who we are talking about cannot hurt somebody,тАЭ Merce said.
Some of the prisoners staying at the Halawa infirmary in June couldnтАЩt walk or dress themselves. One man couldnтАЩt recall what his illness was. Another with brain cancer couldnтАЩt coherently respond to questions.
Sean Sanada, the O╩╗ahu Region CEO with the Hawai╩╗i Health Systems Corp., oversees the regionтАЩs two state-funded long-term care facilities, Leahi Hospital and Maluhia. Sanada said that the health system has reviewed dozens of compassionate release referrals but has never accepted any of them.
Sanada said the facilities donтАЩt discriminate based on where the resident comes from. His main concerns, he said, were his staffтАЩs safety and the lack of resources to adequately care for the patient.
тАЬThe risk is just too high in most of those instances,тАЭ Sanada said.
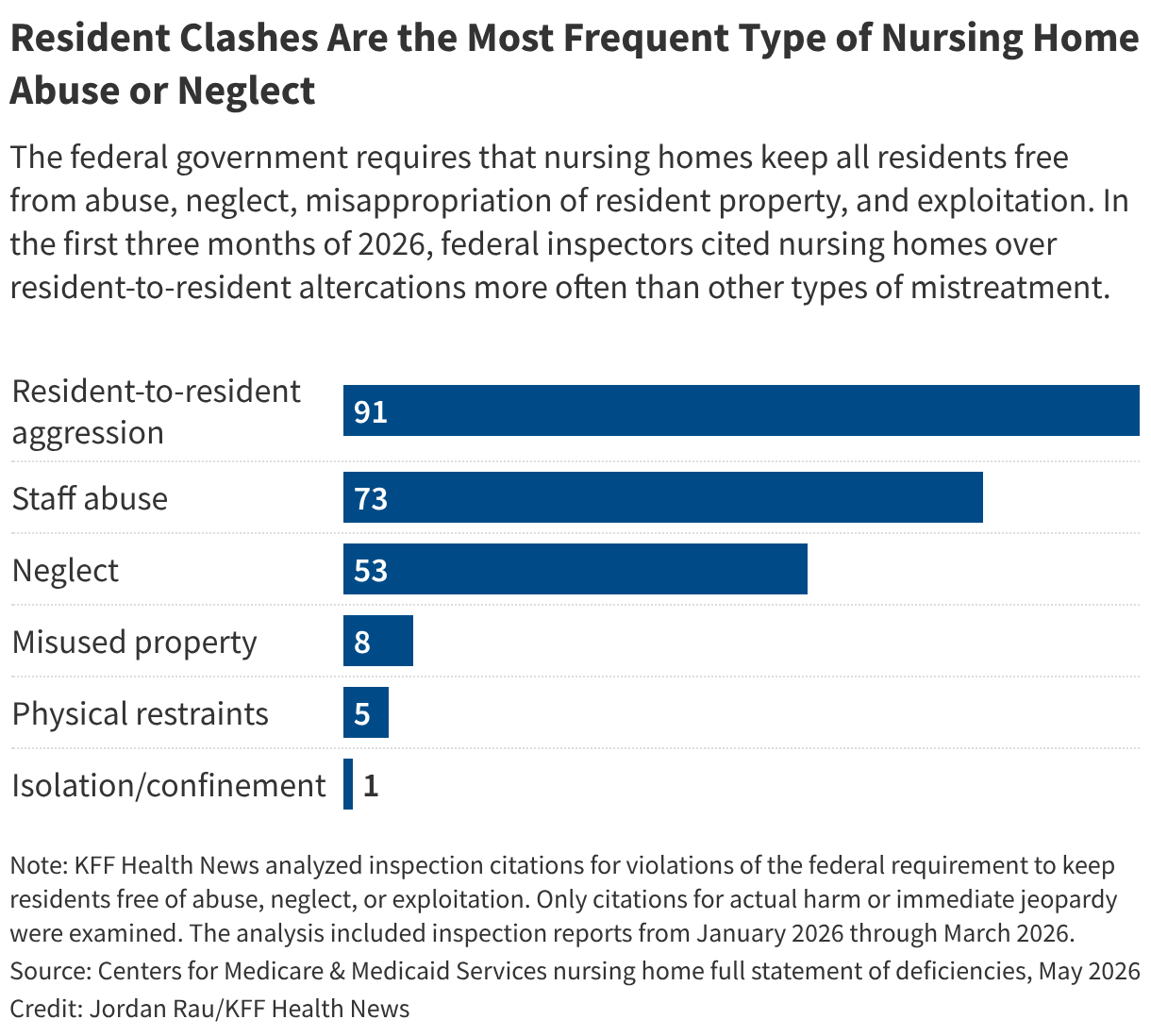
Violent incidents in long-term care facilities have been well documented. A observing 14 assisted living facilities found that in just one month, 15% of residents experienced resident-to-resident aggression.
When long-term care facilities refuse to accept prisoners who have been granted compassionate release, it leaves state taxpayers footing a larger bill. The annual cost to incarcerate an individual in ▒с▓╣╖╔▓╣╛▒тАШi with complex needs is up to eight times the $112,505 average of housing one person in prison, according to FAMM. In comparison, the average Medicaid reimbursement for a long-term care patient at a Hawai╩╗i Health Systems Corp. facility is about .
Even after being granted compassionate release, prisoners who cannot find placements at long-term care facilities can wait for months or longer in the infirmary at the Halawa Correctional Facility in Honolulu. (Ashley Mizuo/║┌┴╧│╘╣╧═Ї News)
Four states тАФ Connecticut, Georgia, Massachusetts, and Vermont тАФ contract with nursing facilities to take prisoners who are granted compassionate release, according to FAMM.
The iCare Health NetworkтАЩs MissionCare Health, which operates nursing homes for people coming out of prison, secured contracts in three of those states. David Skoczulek, iCareтАЩs vice president of business development and communication, estimated that its rates are $100 to $350 a day more per patient than the average nursing home rates in the states where they operate.
In Hawai╩╗i, the correctional department determines recommendations to send to the parole board, which decides whether to grant the release. Prisoners who are granted the early probation can be released to family members who commit to caring for them or to a long-term care facility.
Corey Reincke, head of the Hawai╩╗i Paroling Authority, said that in his 24-year career he couldnтАЩt recall getting anyone placed into a long-term care facility without family intervening, for instance by contacting facilities themselves.
тАЬParole has to find a facility that can meet their medical needs and is also willing to take them,тАЭ Reincke said. тАЬThatтАЩs where weтАЩre hitting the roadblocks.тАЭ
For one parolee, Reincke called more than 100 care homes, he said, but they all declined to accept the patient, over safety concerns. According to a 2024 state report, while Hawai╩╗iтАЩs long-term care facilities use about workforce strains make it difficult to maintain even those levels.
Hawai╩╗i PrisonersтАЩ Refuge: Family
Last year, 69-year-old Paul Kupihea died at a hospital five days after the state granted him compassionate release to his family. He died before he could get on a flight to his home island.
In July 2025, Lahela Kruse, the mother of KupiheaтАЩs child, received a call from a Honolulu hospital informing her that his condition had become severe. By then he had been diagnosed with an incurable form of cancer and had been in and out of the hospital while still in custody.
Kruse and their daughter flew to O╩╗ahu to see him and were shocked when they saw how sick he was. Their daughter agreed to take him into her home in Hilo, on Hawai╩╗i Island, despite not having a relationship with him for most of her life.
тАЬShe knew he was sick,тАЭ Kruse said. тАЬI told her that, but she didnтАЩt know the severity of it. I didnтАЩt truly know.тАЭ
Her daughterтАЩs willingness to take him prompted his compassionate release. But Kruse said the notification about KupiheaтАЩs illness came too late.
FAMMтАЩs Crane has been working on expanding compassionate release laws in states to allow for more prisoners to qualify and strengthen transparency in the process. Hawai╩╗i lawmakers have tried for years to pass bills on compassionate release, but none has succeeded.
Crane said without a law that outlines a formal process and who qualifies, even family support isnтАЩt enough. Prisoners can still face life-threatening delays, she said.
тАЬThe absence of a compassionate release statute means that people who need compassionate release languish and even die in prison,тАЭ Crane said.
Because Medicaid does not cover healthcare in prisons like the Halawa Correctional Facility, the high cost of care for sick prisoners is left to state taxpayers. (Ashley Mizuo/║┌┴╧│╘╣╧═Ї News)
In AlamedaтАЩs cell, two beds stood about 3 feet apart, with a seatless metal toilet in the corner and a window looking out on a concrete wall. The smell of bleach permeated the room. Alameda said he hoped to see his daughter soon. She recently turned 5.
тАЬI made some mistakes in my life,тАЭ said Alameda, who has been incarcerated since 2024 for drug possession, driving a stolen vehicle, and jumping bail. тАЬI tried when my daughter was born, but I know IтАЩll change, because she needs me out of here.тАЭ
Merce, the former attorney, is still trying to find a place for Alameda, who committed no violent crimes. Merce became aware of prisonersтАЩ struggles through his work as a trial lawyer. He said he has helped about 15 prisoners leave Hawai╩╗i correctional facilities for medical treatment.
He said heтАЩs seen cases in which people have waited years to get out.
тАЬThe ones that stick with me, though,тАЭ Merce said, тАЬare the ones that I never found placements for.тАЭ
Leadership Vacuum: Agencies in New York and Beyond Pass the Buck on Opioid Cash Oversight
Alexis PleusтАЩ son Jeff Dugon died of a heroin overdose in 2014 at age 28. She says his addiction began in high school, when he was prescribed opioid painkillers for a knee injury. In 2023, Pleus protested outside the Supreme Court while justices heard a case about Purdue Pharma, the company many people consider a driver of the opioid crisis. (Mia Hause)
Companies accused of recklessly marketing and distributing prescription opioid painkillers are paying to settle lawsuits over their role in fueling the addiction crisis. ItтАЩs a pot of gold eyed by addiction treatment providers, companies creating the latest opioid-related products, and government officials struggling to balance budgets.
Nearly half of that money is , to be distributed by county commissioners and city councilors. The idea is that local leaders know their communities best and can do justice to these payouts, often described as тАЬblood moneyтАЭ by people whoтАЩve lost loved ones to an overdose.
But many local leaders have little to no training in addiction policy and may lack robust local health departments and policy guardrails to assist them.
That has resulted in spending decisions that many clinicians, researchers, and addiction recovery advocates say are unlikely to save lives or treat substance use disorders.
In New York, where is directly controlled by local governments, counties have spent tens of thousands of dollars on surveillance cameras, technology to help police access data on locked cellphones, and goggles that simulate being drunk, according to public records obtained by the nonprofit advocacy group and shared exclusively with ║┌┴╧│╘╣╧═Ї News. Though the purchases were likely legal, many people consider them a slap in the face because they donтАЩt directly help people struggling with addiction or their families.
Without oversight, counties have the chance тАЬto go rogueтАЭ with this money, said , director of drug policy at VOCAL-NY, an advocacy organization that is tracking settlement money as part of its mission to serve people affected by the war on drugs.
Email Sign-Up
Subscribe to ║┌┴╧│╘╣╧═Ї News' free weekly newsletter, "The Week in Brief."
When advocates and families of overdose victims raise concerns to the various state agencies that could hold localities accountable, those agencies often punt to one another, Budnella and other local advocates said.
It feels тАЬlike the where itтАЩs like everybodyтАЩs pointing at each other,тАЭ Budnella said. тАЬSomebody needs to be able to have the stick and slam their hand on the table and be like, тАШYouтАЩre doing this wrong and this is the consequence.тАЩтАЭ
The experience in New York provides a microcosm of regulators evading oversight responsibility nationwide while varied interests vie for the financial windfall.
ItтАЩs unclear who should тАФ or will тАФ take action on such expenditures that many people harmed by the crisis consider questionable.
In each state, control of the money is split among various entities, creating a leadership vacuum. The federal government . Advocates and families whoтАЩve lost loved ones have pushed for accountability but have limited power. A few states have passed new laws, but change is slow and uneven.
The require the majority of the money to be spent on тАЬopioid remediation,тАЭ with . But the list is broad and open to interpretation. Further complicating the issue, many states тАФ including New York тАФ designate some portion of the settlement dollars as unrestricted, which allows for general spending.
тАЬWe really are wasting this opportunity to use these funds to turn the epidemic around,тАЭ said , a Binghamton, New York, resident, whose 28-year-old son, Jeff Dugon, died of a heroin overdose in 2014.
Jeff Dugon (right) spent Easter with his mother, Alexis Pleus, and brothers in 2014. He died four months later of a heroin overdose. Now, Pleus is fighting to ensure opioid settlement money is spent in ways that can spare other families such heartache. (Mitchell Sosnicki)
He was a chef who loved to rib Pleus about her bad knife skills. She thinks of him and smiles every time she peels garlic the way he taught her. If the money could spare other families such heartache, that would give her solace.
тАЬWe need oversight,тАЭ said Pleus, who runs a nonprofit that is receiving opioid settlement cash from her county to serve people who use drugs and provide support groups for families.
In New York, there are three prime watchdog contenders: the Office of Addiction Services and Supports, the attorney general, and the comptroller.
The Lead State Agency
New YorkтАЩs opioid settlement documents designate the as the тАЬ.тАЭ
It distributes a portion of settlement dollars via grants, according to recommendations from the stateтАЩs . It also has the power to тАЬengage in oversight and audits of projects and programsтАЭ funded by settlement cash and тАЬmay withhold future fundsтАЭ from local governments that do not comply with certain requirements, according to the agreement.
Agency spokesperson Jerry Gretzinger told ║┌┴╧│╘╣╧═Ї News the office has not yet exercised its power to withhold funds but understands its oversight role.
тАЬOASAS has a duty to ensure these funds are used responsibly and strategically to build programs that will have a lasting impact in reversing this crisis,тАЭ Gretzinger wrote in a statement.
The office is currently auditing 19 local governmentsтАЩ use of the money to ensure compliance with тАЬreporting and recordkeeping requirements,тАЭ he said. However, that may not encompass the broader question of whether money was spent on appropriate uses, which many advocates want addressed.
Some people are frustrated with the narrow role OASAS has carved out.
For example, required local governments for the first time to publicly report how they spent settlement money. OASAS on its site. But it does not review the accuracy or detail of that data, instead relying on тАЬthe information as it is providedтАЭ by localities, Gretzinger said.
тАЬThat doesnтАЩt feel like oversight,тАЭ said , a deputy director at the Legal Action Center, which obtained public records about local spending in New York.
Members of the stateтАЩs Opioid Settlement Fund Advisory Board have also to provide more data and evaluation of how dollars are being used. But at a , OASAS Commissioner Chinazo Cunningham deflected.
тАЬOASAS has no oversight over these portions of dollars,тАЭ she said of the 46% of settlement money that goes directly to counties and cities. тАЬIn terms of what kind of data each county collects,тАЭ she added, тАЬwe cannot dictate exactly what that information is.тАЭ
Click for Examples of spending decisions
Local Spending ThatтАЩs Fueling Calls for Oversight in New York
To uncover how opioid settlement cash is being spent, the nonprofit advocacy group filed public records requests with 56 New York counties and New York City, all of which are to disburse as they see fit.
Many of the responses showed spending on addiction treatment, recovery, and prevention initiatives that researchers and clinicians agree are a good use of money. Others surfaced questionable expenditures.
, for example, showed $150,000 in settlement cash directed to тАЬSheriff JailтАЭ with no further description. The county did not respond to repeated inquiries for more details.
Sullivan County spent more than $30,000 on Cellebrite technology, used to extract data from cellphones, and more than $37,000 on Tasers. Though county officials didnтАЩt respond to requests for comment, explained that those purchases came from unrestricted funds.
Such justifications rankle some families affected by the crisis, who say even if there arenтАЩt legal restrictions on those dollars, there should be moral ones.
тАЬAnything that is not directly tied to people who are struggling with opioid addiction or the loss of someone is a poor use of funds,тАЭ said , who lost a son to an overdose and now runs a nonprofit aimed at helping families dealing with addiction. Her organization has received settlement funds from Broome County, New York.
Alexis Pleus is pictured with her son Jeff Dugon in 2003, when he was 17. She thinks of him every time she sees a sunrise or sunset. He loved them and would often send her photos, she says. (Jason Dugon)
Records also revealed that many jurisdictions have yet to spend a significant portion of their money тАФ a other .
Local officials say thoughtful planning takes time. But some advocates suspect ulterior motives. Millions of settlement dollars in bank accounts can generate sizable interest.
In March, it came to light that Nassau County had in interest accrued from unused opioid settlement funds to the countyтАЩs general fund, where it could be used for any purpose. County officials didnтАЩt respond to requests for comment. The money was following public backlash.
Advocates suspect such attempts are happening elsewhere but are difficult to identify within complex budgeting documents.
It feels like тАЬitтАЩs up to us all тАФ the organizers, the advocates, the service providersтАЭ тАФ to be constantly watching, said , director of drug policy at the advocacy organization VOCAL-NY. тАЬItтАЩs frustrating.тАЭ
ThatтАЩs why state agencies are being called on to step into an oversight role.
The Top Law Enforcement Officer
New York has been one of the leading national voices on prosecuting pharmaceutical companies that fueled the overdose crisis. Her office has issued on the topic, touting her role in securing billions of opioid settlement dollars for the state.
But when asked about the attorney generalтАЩs role in ensuring this windfall is spent appropriately, her office passed the buck to other agencies.
тАЬWhile our partners in state and local governments distribute and oversee these funds, we will continue our work to hold accountable the companies responsible for fueling the spread of addictions and overdoses,тАЭ spokesperson Grant Fox wrote in a statement.
That stance contrasts starkly with many peopleтАЩs views of the officeтАЩs responsibility.
A state senator, a member of the opioid settlement advisory board, and several advocates named the attorney generalтАЩs office as a key enforcement entity.
тАЬThe money is here because of their efforts,тАЭ said Democratic state , who chairs the committee on alcoholism and substance use disorders and has introduced of related to settlement funds. тАЬI believe it is under the Office of the Attorney General to enforce.тАЭ
Budnella, the advocate with VOCAL-NY, agreed, saying, тАЬIt would be a shame for all of their work that they have done to secure all this funding for it to be misspent.тАЭ
VOCAL-NY is a statewide advocacy organization that tracks opioid settlement money as part of its mission to serve people affected by the war on drugs. The group is calling on state agencies to hold city and county officials accountable to ensure the money is spent on services that help people with substance use disorders and their families. (VOCAL-NY)
Attorneys general in and have taken more active roles, issuing lists of ways opioid settlement money cannot be spent. The lists include many law enforcement expenditures that have raised concerns for advocates in New York.
JamesтАЩ office did not respond to a specific question about whether sheтАЩd consider creating a similar list.
The Fiscal Watchdog
Some people have suggested that the state comptroller, as a steward of New YorkтАЩs finances, could play an oversight role, perhaps by conducting or requiring audits.
Early this year, the Reason Foundation, a libertarian think tank, that would create audit requirements for organizations receiving settlement cash. The blueprint suggests recipients of more than $1 million in opioid settlements be required to undergo an independent review of financial statements and transaction testing to determine whether funds were used for their intended purpose. Smaller grantees, receiving less than $1 million, could simply provide an unaudited accounting of the funds.
ItтАЩs тАЬnot telling states what is and what isnтАЩt an appropriate use,тАЭ said , a co-author of the Reason Foundation plan. тАЬWeтАЩre simply trying to ensure recipients follow through with their promises.”
No state has adopted the model law yet. But the office of New York told ║┌┴╧│╘╣╧═Ї News it is already conducting an audit.
The process, which began in February, тАЬis looking at OASASтАЩ oversightтАЭ of the opioid settlement money, said spokesperson Mary Mueller. It includes settlement money controlled by the state and local governments.
Mueller said any future enforcement action тАЬwill depend on the results of our current work and our ongoing monitoring.тАЭ
The office is following in the footsteps of comptrollers and auditors in , , and , Tennessee, who have taken action on settlement cash.
These initial steps have given some advocates and researchers hope for the future of opioid settlement dollars, which are expected to flow for more than a decade.
тАЬWeтАЩre already years in and weтАЩve seen the craziest storiesтАЭ of this money and a , said , a co-author of the Reason FoundationтАЩs model law. тАЬIf we can prevent that at least a little and have these funds be a bit more focused, I donтАЩt think itтАЩs too late.тАЭ
A Deloitte-Run System Denied Medicaid Benefits for MichiganтАЩs Disabled. Now TrumpтАЩs Law Piles On.
A Deloitte-Run System Denied Medicaid Benefits for MichiganтАЩs Disabled. Now TrumpтАЩs Law Piles On.
After Marie Noon was wrongly denied Medicaid coverage by MichiganтАЩs benefits system, she paid hundreds out-of-pocket for medications she takes each day to manage her rare disease. (Kate Wells/║┌┴╧│╘╣╧═Ї News)
A Deloitte-Run System Denied Medicaid Benefits for MichiganтАЩs Disabled. Now TrumpтАЩs Law Piles On.
Marie Noon takes eight medications a day. One keeps her heart rate from spiking to avoid a stroke. One prevents debilitating headaches. Another ensures she doesnтАЩt retain excess fluid.
More than a decade ago, Noon said, she was diagnosed with adult-onset StillтАЩs disease, a rare type of inflammatory arthritis that can cause rashes, debilitating pain, and fevers. The disease upended her life.
She had been living a typical suburban life in Michigan, shuttling her two kids to activities like cheerleading, choir practice, and track. She was active in the PTA. She managed a bank.
She went from that to crawling to the bathroom because she was in so much pain, тАЬjust crying all day longтАЭ from being so sick.
Noon, who is disabled, said she couldnтАЩt work for eight years тАФ a time marked by hospital stays that stretched for weeks.
тАЬI honestly thought I was going to die,тАЭ Noon said.
So it was a shock when Michigan denied her application for Medicaid benefits last year after she lost private insurance. Worse yet, it came down to an IT error, according to an attorney who helped Noon overturn the denial.
тАЬI canтАЩt afford my medical care. I have to have insurance,тАЭ said Noon, who has returned to working.
Deloitte, a multibillion-dollar global consulting firm, has operated MichiganтАЩs Medicaid eligibility system under contracts worth roughly $768 million since 2006, according to contracts reviewed by ║┌┴╧│╘╣╧═Ї News. Nationwide, Deloitte dominates this important slice of government business: At least 25 states have awarded the company contracts to build or run computer systems that control access to safety net benefits such as Medicaid.
MichiganтАЩs system has incorrectly directed people with disabilities into skimpier benefits that cover limited care or has denied coverage completely, a ║┌┴╧│╘╣╧═Ї News investigation found. Similar problems were at the center of a class-action suit in Tennessee, , and have occurred in Texas, according to interviews and state records.
The ║┌┴╧│╘╣╧═Ї News investigations are based on statements from state officials, allegations and declarations in court documents, emails obtained through public records requests, state government information provided to Medicaid enrollees and applicants, and interviews with attorneys and patients or their caregivers.
In an emailed statement, Deloitte spokesperson Karen Walsh said it found тАЬno system anomalies causing routine denials of Medicaid for people with disabilities.тАЭ
тАЬThere are many reasons why someone may no longer be eligible for a benefit they once received or believe they deserve,тАЭ Walsh said. тАЬAll of the eligibility systems we support are owned by the states and built to their unique specifications. We will continue to work at the direction of our state clients.тАЭ
Lynn Sutfin, a spokesperson for MichiganтАЩs Department of Health and Human Services, said it “is not aware of any widespread or systemic issuesтАЭ within Bridges, MichiganтАЩs eligibility system for Medicaid, SNAP, and other benefits, тАЬrelated to disabilityтАСbased eligibility pathways.”
Since 2006, Deloitte’s contracts with the state have said the company is responsible for development, implementation, maintenance, operations, and enhancements to the Michigan system.
Computer system problems foreshadow trouble as states prepare to roll out the most significant and complicated changes to their Medicaid programs in years. Those changes, dictated by President Donald TrumpтАЩs landmark One Big Beautiful Bill Act, have states rushing to update their Medicaid computer systems.
Nationwide, on Medicaid have a disability, according to KFF.
тАЬWhen these administrative systems get overloaded, everyone gets impacted,тАЭ said Pamela Herd, a University of Michigan professor who researches bureaucratic obstacles to accessing government benefits. тАЬThe systems are going to be really, really strained.тАЭ
In Michigan, Noon was eligible for Medicaid through a program that provides coverage to disabled adults who work. But the stateтАЩs computer system didnтАЩt register that she is disabled and said she earned too much to qualify, according to documents reviewed by ║┌┴╧│╘╣╧═Ї News and interviews with Noon and Anastassia Kolosova, a disability rights attorney who helped her.
Without Medicaid coverage, Noon paid hundreds of dollars out-of-pocket for prescriptions, after scrounging for discount coupons. She takes some of the drugs twice a day.
Without them, тАЬIтАЩm toast,тАЭ she said. It was stressful тАЬnot knowing if my medicineтАЩs going to be $50 or $500 this month, because it changes constantly.тАЭ
Noon said her doctor agreed to fewer visits to avoid medical bills.
тАЬIt was kind of a nightmare,тАЭ Noon said.
Email Sign-Up
Subscribe to ║┌┴╧│╘╣╧═Ї News' free weekly newsletter, "The Week in Brief."
тАШI Just Wanted To Give UpтАЩ
Medicaid, a safety net health program jointly run by the federal government and states, people with low incomes or disabilities. State governments rely on companies like Deloitte to design and operate computer systems that assess whether people qualify for Medicaid or food aid through the Supplemental Nutrition Assistance Program, commonly known as food stamps.
That technology has a history of errors that deprive eligible people of benefits, earlier ║┌┴╧│╘╣╧═Ї News investigations have shown. As reported previously, Kenneth Smith, a Deloitte executive who leads its national human services division, said Medicaid eligibility technology is state-owned and agencies тАЬdirect their operationтАЭ and тАЬmake decisions about the policies and processes that they implement.тАЭ
тАЬTheyтАЩre not Deloitte systems,тАЭ he said, noting Deloitte is one player among many who together administer Medicaid benefits.
States are under immense pressure to update their eligibility systems on a tight schedule to adhere to requirements in the RepublicansтАЩ sweeping 2025 tax and spending law. Companies including Deloitte, Accenture, and Optum are being paid millions in taxpayer funds to make the changes, which are projected to strip Medicaid from roughly 7.5 million people and SNAP from 2.4 million people by 2034.
Many coverage restrictions in the new federal law donтАЩt apply to seniors, children, or people who are disabled, such as Noon. Nonetheless, the lawтАЩs demands on state agencies and the computer systems they oversee will disrupt benefits, advocates for Medicaid enrollees and other healthcare experts said in interviews.
The same systems also need to correctly classify why someone is eligible for Medicaid тАФ and therefore which rules and restrictions apply.
The lawтАЩs SNAP restrictions began to take effect in 2025, and major Medicaid provisions begin later this year, generally after the midterm elections.
Kolosova is a supervising attorney with Disability Rights Michigan, a legal advocacy organization for people with disabilities. She said she has been unable to get a meeting with Michigan officials to understand the underlying problem that deprived Noon of health coverage.
Anastassia Kolosova, a supervising attorney with Disability Rights Michigan, helped Noon navigate the complicated process to obtain safety net health insurance through Medicaid. Kolosova says she has seen multiple wrongful coverage denials and fears problems will soon get worse because of changes required by federal law. (Kate Wells/║┌┴╧│╘╣╧═Ї News)
State records show Deloitte has held contracts for at least 14 years for Bridges, MichiganтАЩs eligibility system for Medicaid, SNAP, and other benefits. In its attempts to secure more business, the company often cites its nationwide footprint in Medicaid operations.
тАЬDeloitte understands Bridges,тАЭ and its history in Michigan makes the company тАЬthe ideal vendor,тАЭ the firm said in its . Given ╢┘▒Ё▒Є┤╟╛▒│┘│┘▒ЁтАЩs work on similar systems in 31 other states, , тАЬMichigan benefits from our technical expertise drawn from across the nation.тАЭ
But advocates who work with people with disabilities say MichiganтАЩs computer system has failed to recognize when certain adults should receive Medicaid benefits.
Problems arenтАЩt unique to the Great Lakes State. Medicaid beneficiaries who brought a against Tennessee in 2020 said the stateтАЩs Deloitte-built system тАЬdoes not reliably test for eligibilityтАЭ for several categories of people with disabilities. The firmтАЩs is worth $1.12 billion over a decade.
A federal judge in 2024 , ruling that Tennessee violated federal law and the U.S. Constitution. The lawsuit does not name Deloitte as a defendant.
In Michigan, a from the stateтАЩs Office of the Auditor General said government agencies тАЬdid not provide effective project administrationтАЭ and failed to ensure that the state could тАЬindependently maintain and operate BridgesтАЭ because тАЬthe contractor did not transfer knowledge and skillsтАЭ to state officials, according to the audit.
The auditorтАЩs report said that, as a result, ╢┘▒Ё▒Є┤╟╛▒│┘│┘▒ЁтАЩs original contract тАФ valued at roughly $70 million тАФ ballooned by $50 million over the initial cost, a 71% increase. State records show Michigan would go on to add millions more, bumping the cost of ╢┘▒Ё▒Є┤╟╛▒│┘│┘▒ЁтАЩs initial contract to $124.1 million.
The audit said maintaining the contract would result тАЬin significant additional costs.тАЭ
Sutfin said that тАЬthe state is now fully capable of operating and maintaining Bridges independently.тАЭ
╢┘▒Ё▒Є┤╟╛▒│┘│┘▒ЁтАЩs in Michigan тАФ worth $197.4 million тАФ is set to expire in 2030.
Noon applied for Medicaid in August, she and Kolosova said. In September, the Michigan Department of Health and Human Services sent a notice denying her coverage, citing incorrect income information and stating she wasnтАЩt disabled, according to Kolosova and state documents reviewed by ║┌┴╧│╘╣╧═Ї News.
Noon said that when she called the state for help, state workers тАЬdidnтАЩt know anything aboutтАЭ the Medicaid program she had applied to, Freedom to Work.
тАЬI canтАЩt tell you how many times I just wanted to give up,тАЭ she said.
For some people with disabilities, Medicaid is supposed to count only half their earnings when assessing whether they should receive benefits. That didnтАЩt happen. Kolosova said she thinks MichiganтАЩs eligibility system didnтАЩt identify Noon as disabled, even though the state тАЬalready had all the information they neededтАЭ to show she was.
By failing to recognize her disability, the state used the wrong income formula and said Noon earned too much to qualify for Medicaid, she added. Deloitte and Michigan declined to respond to a detailed list of questions about NoonтАЩs experience.
Kolosova said Disability Rights Michigan has seen a growing number of calls from people about Freedom to Work benefit denials. тАЬMaybe two or three a month,тАЭ she said.
тАЬThereтАЩs something wrong with the system if theyтАЩre relying on individual caseworkers to catch this,тАЭ Kolosova said. тАЬThe system needs to work.тАЭ
Noon at home with her dog, Ziggy. Despite being eligible for Medicaid, she was denied coverage in 2025 because of an error with the stateтАЩs benefits system. It took months of pushback before the state reversed its mistake. Even as a тАЬtech-savvyтАЭ former bank manager, she says, she wanted to give up several times along the way. (Kate Wells/║┌┴╧│╘╣╧═Ї News)
Enrolled in the Wrong Coverage
NoonтАЩs experience isnтАЩt the first time in recent years that people with disabilities have been denied benefits by Deloitte-run eligibility systems.
In Texas in 2023, Lilly Livingston, who has Down syndrome and is now 22, was abruptly cut off from Medicaid benefits, according to LivingstonтАЩs mother, Marie. She has undergone numerous surgeries to reconstruct her severely misaligned jaw, which caused sleep apnea and impaired her speech and chewing ability. She relied on an array of Medicaid services, including speech and occupational therapy.
When Livingston lost benefits, she was wrongly enrolled in Healthy Texas Women, a limited program that provides breast and cervical cancer screenings and family planning services.
тАЬTrying to fix that was a nightmare,тАЭ Marie Livingston said.
Terry Anstee, an attorney with Disability Rights Texas, intervened.
In a September 2023 email with the subject line тАЬURGENT,тАЭ Anstee begged a Texas Medicaid eligibility worker for help.
Some unknown тАЬerrorтАЭ had occurred and stripped Livingston of her benefits, Anstee said in an email he sent to a state Medicaid staffer. тАЬLilly has had 2 major surgeries, and her recovery is contingent on Medicaid.тАЭ
It was clear that Livingston qualified for Medicaid through multiple paths, Anstee said: тАЬIt never made any sense.тАЭ
Deloitte declined to respond to a detailed list of questions about LivingstonтАЩs case. Jennifer Ruffcorn, a spokesperson for Texas Health and Human Services, confirmed that Livingston was erroneously enrolled in Healthy Texas Women. However, Ruffcorn said, Livingston did not experience a lapse in Medicaid coverage in 2023.
Anstee disputed the stateтАЩs characterization: тАЬA glance in the system by a Texas HHS press officer or other staff 3 years after the fact may not tell the full story or show the issues that Ms. Livingston endured in August and September 2023. Ms. Livingston experienced lapses in coverage.тАЭ
The problem Livingston encountered in Texas was also reported in Michigan.
In 2024, mental health services advocates in Michigan raised red flags about a similar error: People with disabilities were being enrolled in a limited Medicaid program covering sexual health and family planning services. Plan First covers only services and treatment for sexually transmitted infections. It doesnтАЩt provide the comprehensive coverage that people with disabilities require.
But some enrollees were тАЬbeing automatically enrolled in Plan First,тАЭ Malcolm Kletke, a lobbyist representing the Community Mental Health Association of Michigan and other mental health providers, wrote to a Michigan health official, according to emails obtained by ║┌┴╧│╘╣╧═Ї News through a public records request.
These enrollees had тАЬlong received Medicaid due to their disability,тАЭ and getting enrolled in the wrong plan meant losing access to тАЬservices essential to their recovery and quality of life,тАЭ Kletke wrote in September 2024 to Amy Epkey, a senior deputy director of the Michigan Department of Health and Human Services.
In fact, the stateтАЩs own records show that Medicaid enrollment for those with disabilities did decline.
Over roughly four years, enrollment in the Medicaid category that includes people with disabilities , according to the Michigan House Fiscal Agency, which provides nonpartisan analysis to lawmakers. The drop was unusual given people generally leave the program because of death or having recovered from a temporary disability, and itтАЩs unlikely those numbers would balloon, said Robert Sheehan, who was the mental health associationтАЩs CEO at the time.
Sutfin said the state examined the decline in enrollment and found тАЬseveral contributing factors, including postтАСcovid renewal patterns, changes in beneficiary circumstances and movement to other coverage categories.тАЭ
After inquiries from ║┌┴╧│╘╣╧═Ї News, the Michigan health department acknowledged in April that it had made changes to тАЬaddress concerns raised by advocates.тАЭ
MichiganтАЩs computer system now prevents approval of Plan First benefits until all other coverage options are evaluated, Sutfin told ║┌┴╧│╘╣╧═Ї News. Sutfin said the changes were implemented but тАЬnot to correct system errors.тАЭ
Sutfin said the state submitted a change request to Deloitte to address this problem. The fix was implemented in January 2025.
Until presented with KletkeтАЩs email, the state had denied there were problems related to Plan First.
Even after the state addressed that issue, other problems persisted.
NoonтАЩs coverage denial notice arrived in September. She fought with the state for months to reverse its decision, тАЬpaying cash for all of the medicines through these appeals over and over and over again.тАЭ
It was only in January that she was approved.
тАЬI literally cried,тАЭ Noon said. тАЬIt was a really big deal.тАЭ
Doctors тАШCringeтАЩ at Possibility of Documenting Which Medicaid Enrollees Too Sick To Work
Doctors тАШCringeтАЩ at Possibility of Documenting Which Medicaid Enrollees Too Sick To Work
Alice Thornton has spent more than two decades treating people living with HIV in Lexington, Kentucky.
Her team tends to тАЬcringeтАЭ anytime they hear about patients having to fill out lots of paperwork, like when applying for Social Security Disability payments, because it can be a difficult, burdensome process.
Thornton tries to support her patients, she said, but understands the limits of her training.
тАЬA lot of times the forms are so complex that I don’t really know what’s the true definition of what this form is asking me,тАЭ she said. тАЬWe refer them to a disability provider.тАЭ
Doctors including Thornton worry theyтАЩll see more of those kinds of requests because of coming changes to Medicaid, the government health insurance program for people with low incomes or disabilities. Starting Jan. 1 in most of the country, some enrollees тАФ mainly adults without dependents тАФ must prove theyтАЩre working or performing other qualifying activities 80 hours a month.
issued in June say people can obtain an exemption if theyтАЩre тАЬmedically frail,тАЭ or too sick or disabled to work, which may require them to submit documentation from a medical professional. That standard prompted a lawsuit at the end of June from dozens of mostly Democratic-led states and has Thornton worried it could force her and her staff to assess things like how much a patient can lift or how far they can walk.
тАЬIf I’m asked, тАШIs this person medically frail?тАЩ What does that even mean?тАЭ Thornton said. тАЬI donтАЩt know, and IтАЩve been doing this for 25 years.тАЭ
Last yearтАЩs GOP tax-and-spending law known as the One Big Beautiful Bill Act established the work rule, which will affect an estimated when more states start enforcing it. The mandate is expected to cause a larger increase in the number of people without health insurance than any other part of the law, a health information nonprofit that includes ║┌┴╧│╘╣╧═Ї News.
Doctors say they arenтАЩt trained to accurately assess whether someoneтАЩs health keeps them from working. Many donтАЩt have time to handle another administrative task that takes them away from patient care. And being involved in whether someone gains access to a public benefit undermines the doctor-patient relationship, several doctor groups and physicians said.
тАЬWhen you introduce unnecessary, non-evidence-based, confusing, and bureaucratic policies like this into clinical care, it just raises the level of moral distress for providers,тАЭ said Christopher Chen, a senior healthcare adviser at the consulting firm Manatt.
The Centers for Medicare & Medicaid Services declined to respond on the record about doctorsтАЩ concerns. But the agency confirmed that enrollees may need to get documentation from a clinician to prove theyтАЩre too sick to work and said states would make final determinations.
The Trump administration has previously said states should use available data sources тАФ such as medical claims and payment data тАФ before making patients submit proof of medical frailty from a provider.
тАЬDocumentation should be relatively easy to provide,тАЭ Mehmet Oz, the CMS administrator, said during a June 1 press call.
But deciding whether a patient is too sick to work is a subjective, high-stakes decision, said Chen, who also practices as a hospitalist at Valley Medical Center in Renton, Washington.
“We’re trained to take care of people,тАЭ he said. тАЬWe’re trained to learn about someone’s symptoms, make diagnoses, treat them. We’re not trained to make these kinds of work determinations.тАЭ
When they apply and every six months after, Medicaid enrollees subject to the rule will have to prove that theyтАЩre performing the minimum monthly hours of qualifying activities тАФ or will likely have to prove as frequently that they qualify for an exemption.
If states canтАЩt find sufficient evidence that someone is too sick to work, that person will be able to self-attest to it under penalty of perjury тАФ but only for a short time. States may take someoneтАЩs word that theyтАЩre medically frail twice in 2027 and only once in 2028.
Last month, 25 mostly Democratic-led states over the final regulations, arguing the medical frailty standard would be too hard for enrollees to meet тАФ and for states to assess.
The standard, they argue, requires state Medicaid agencies to тАЬtake on the role of occupational medicine expertsтАЭ or adds that burden to physicians who are not necessarily trained in occupational medicine.
CMS declined to comment on the litigation.
The Trump administration has crusaded against fraud in government health programs including Medicaid. It recently тАФ including medical professionals тАФ over more than $6.5 billion in alleged fraud schemes.
CMS has said it will keep a close watch on how states administer the work requirements and may take corrective action if states step out of line.
That has doctors concerned about the potential repercussions if they incorrectly assess whether someone is too sick to work, as farfetched as those worries might be, said Rahul Vanjani, a primary care and addiction medicine physician and researcher at Brown University.
тАЬWe, using our imaginations, wonder if someone is auditing these forms in the background and if theyтАЩre going to reach out to the licensing board.тАЭ
The country is short of primary care providers, and it could be hard for people seeking an exemption to find a clinician to help them document that theyтАЩre too sick to work, doctors said.
It will be even more challenging for someone without insurance, said Jennifer Wagner, who researches Medicaid eligibility at the left-leaning Center on Budget and Policy Priorities.
тАЬHow could an applicant who doesnтАЩt have health coverage get a doctorтАЩs note?тАЭ she asked.
The American Medical Association, the nationтАЩs largest professional association of doctors and medical students, lobbied federal officials to change the standard for documenting medical frailty in the days before the final regulations were made public.
In May, the AMA sent to Oz, the CMS administrator, arguing that forcing doctors to attest to their patientsтАЩ ability to work wouldnтАЩt just be an administrative headache but would affect the way they interact with those in their care.
In a statement, the associationтАЩs president, Willie Underwood III, said the work rule тАЬtransforms the clinical encounter into an eligibility gatekeeping process.тАЭ
тАЬPatients will likely sense that shift,тАЭ he said. тАЬAnd if they begin to suspect that what they share with their physician could affect their coverage, the conditions for open and honest communication will start to break down.тАЭ
Doctors have a fixed amount of time to spend with patients and would rather focus on treating medical conditions than filling out forms, especially ones that put them in a position to тАЬrepresent the state,тАЭ said John Ayanian, an internal medicine physician and researcher at the University of Michigan.
тАЬTheir first obligation is to serve the best interest of their patients,тАЭ Ayanian said.
Lauren Davis, an attorney with Community Legal Services of Philadelphia, helps clients navigate other public benefit programs, such as the Supplemental Nutrition Assistance Program, which has a similar work rule. Enrollees can get an exemption from it if theyтАЩre too sick to work.
She recalled a client with a cognitive condition that affected her memory. The clientтАЩs doctor wasnтАЩt comfortable filling out an exemption form without seeing her in person, but she kept forgetting to make an appointment and eventually gave up, said Davis, who worries Medicaid enrollees could face similar barriers to getting exemptions.
тАЬThis person is eligible,тАЭ Davis said. тАЬThe reason that they’re not able to get what they need to show that they’re eligible is because of their medical condition.тАЭ
Violence Repeatedly Erupts at Dementia Care Facilities Despite Warnings, Inspections Show
Rebecca Norton warned officials at her motherтАЩs Minnesota memory care facility that another resident was coming into her motherтАЩs room and harassing her, a state report said. Her mother, Gladys Lynch, was later shoved down by the resident and died five days later, the report said. Her death was ruled a homicide. (Liam James Doyle for ║┌┴╧│╘╣╧═Ї News)
Sam Ato Timaloa, a paroled sex offender who also served time for attempted murder, had dementia and an acute intolerance of noise тАФ especially from roommates at Sunrise Post Acute, a nursing home in Banning, California. Over four months in 2025, a state investigative report found, Sunrise switched TimaloaтАЩs room eight times, the last into one occupied by Attilio Cecchetto, 92, a retired tile installer whose dementia led him to frequently moan, mumble, and yell.
Overnight, a nurse aide walked into their room and saw blood splattered on the floor, walls, and ceiling, according to a grand jury transcript. CecchettoтАЩs face тАЬlooked twisted and smashed,тАЭ the aide testified. A Banning city police officer testified that Timaloa, 77, told him that he had punched Cecchetto twice.
тАЬHe just kept saying that Attilio was being too loud: тАШHe talks too much,тАЩтАЭ the officer said.
Attilio Cecchetto (right), a retired tile installer pictured with his son Gino, often moaned or yelled, a symptom of his dementia. His California nursing home assigned him a new roommate, a former convict whose dementia made him react strongly to noise, a state report said. (Marco Cecchetto)
Cecchetto died two days later from blunt force facial trauma.
тАЬYou get placed in a facility like this to be taken care of, not to be murdered,тАЭ one of his sons, Gino Cecchetto, said in an interview. тАЬThis was completely preventable at many different points.тАЭ
Timaloa pleaded not guilty to assault. The charges were later upgraded to murder, and a judge ordered a mental health evaluation. The judge will rule as early as August on whether Timaloa is competent to stand trial.
PACS Group, the nursing home chain that owns Sunrise, denied negligence. тАЬWe strive to provide quality care to everyone we serve, and our hearts continue to go out to the Cecchetto family for their loss,тАЭ PACS spokesman Brooks Stevenson said in an email.
In nursing homes primarily occupied by impoverished people as well as posh assisted living facilities that cost upward of $10,000 a month, agitated residents have shoved, punched, bit, and kicked others. They have wielded canes, walkers, pens, a plate, a mop stick, a shoe, a belt buckle, and even the footrests of wheelchairs as weapons, federal inspection reports show.
How often these altercations take place nationwide is unknown, but an of 14 assisted living facilities in New York state led by Cornell University researchers estimated 1 in 7 residents experienced aggression within a month, including verbal, physical, or sexual acts. Their of 10 New York state nursing homes estimated 1 in 5 residents experienced an altercation in a month. Researchers have found that these assailants are to have dementia.
The diseases that cause dementia can impair brain circuits involved in impulse control and threat perception, raising the risk of aggressive behavior. Residents with AlzheimerтАЩs disease and other dementias constitute more than living in these settings, many of which include specialized units.
Often, altercations involving a resident with dementia erupt after danger signals are missed or ineffectively addressed, according to a ║┌┴╧│╘╣╧═Ї News examination of court records, police reports, and state and federal inspection reports.
Since the start of 2024, the federal Centers for Medicare & Medicaid Services has faulted nursing homes at least 700 times for failing to protect residents from physical, sexual, or verbal abuse by other residents, CMS inspection reports show. The federal records do not include assisted living facilities, which are regulated by states.
In the first three months of this year, CMS cited nursing homes more often for resident-to-resident abuse than for any other type of abuse, neglect, or exploitation, including abuse by employees, the reports show.
The long-term care industry says not every clash can be averted. Presbyterian Homes & Services, a nonprofit Christian chain of senior living facilities, said in a statement: тАЬCaring for individuals living with advanced dementia is complex, and behaviors can change in ways that are difficult to fully predict or prevent, even with clinical interventions in place.тАЭ
Eilon Caspi, a and researcher who studies resident-on-resident altercations, said that usually there is a specific unmet need that precedes an altercation. тАЬIn the vast majority of incidents,тАЭ he said, тАЬthere are warning signs in the months, weeks, days, hours, and sometimes minutes and seconds prior.тАЭ
Fertile Battlegrounds
One about AlzheimerтАЩs, the most common dementia disease, holds that as the brainтАЩs networks deteriorate, the balance shifts between the prefrontal cortex, which helps govern judgment and self-control, and limbic regions including the amygdala, which helps process fear and threat responses.
As cognition clouds, people lose the ability to understand what is happening around them and to put distress into words, researchers say. Pain, infection, medication side effects, and other physical and emotional distresses through shouting, intimidating gestures, kicking, pushing, or punching. Long-term care facilities can be triggering environments, with intimate care often delivered by a changing stream of aides whom residents canтАЩt recognize. Amid noise, close quarters, and rigid routines, interactions become flash points.
тАЬYou don't feel safe, because you don't know these strangers who are coming in and taking off your clothes,тАЭ said Al Power, a geriatrician and an advocate for alternative models of care for people with cognitive issues. тАЬThese things will be distressing to anybody.тАЭ
Email Sign-Up
Subscribe to ║┌┴╧│╘╣╧═Ї News' free Morning Briefing.
The Cornell researchers found verbal altercations were the most common type of aggressive interaction but estimated 4% of assisted living residents and 5% of nursing home residents in their studies experienced physical assaults in a month.
Another Cornell study found that Connecticut police were called to nursing homes for more often than allegations of staff abuse, theft, and residents wandering away without supervision combined. A national analysis of survey data from the Centers for Disease Control and Prevention calculated in assisted living facilities engaged in physical aggression or abuse toward other residents or staff members.
Many of the physical aggressions ║┌┴╧│╘╣╧═Ї News identified in CMS inspection reports were perpetrated by residents with diagnoses of dementia, schizophrenia, or other cognitive disorders. In some physical altercations, both residents were aggressors, while other fights were one-sided. Sometimes the residents were roommates.
Laura Mosqueda, a geriatrician at the University of Southern CaliforniaтАЩs Keck Medicine in Los Angeles and a senior adviser to the National Center on Elder Abuse, said: тАЬWhat worries me is that we just end up blaming two people who have either cognitive impairment or severe, uncontrolled mental health issues, when theyтАЩre supposed to be in an environment where people are safe.тАЭ
тАШOnly a Matter of TimeтАЩ
Gladys Lynch, a retired department store accountant, transferred into the memory care unit at Harbor Crossing in White Bear Lake, Minnesota, in September 2025. Her monthly cost was more than $10,000, according to an invoice provided by the family.
One of LynchтАЩs daughters, Rebecca Norton, installed web cameras in her room and often saw another resident inside. тАЬEvery day I looked at it, this woman would be walking into my momтАЩs room, harassing her, digging through her things, using her bathroom, yelling at her,тАЭ Norton said in an interview. She informed Harbor CrossingтАЩs administration, and the facility said it would start locking her motherтАЩs door.
Norton emailed a Harbor Crossing administrator a list of issues with her motherтАЩs care. тАЬMy biggest concern,тАЭ she wrote, was that her motherтАЩs door was not consistently locked and the webcam showed the woman had again entered, rummaged through the bathroom, and taken a couple of adult diapers.
A Minnesota investigative report determined Gladys LynchтАЩs memory care home failed to protect her from another resident known for behaving aggressively. тАЬMy mom deserved better than what they gave her,тАЭ says her daughter Rebecca Norton, seen here holding a photo of Lynch. The home has asked the state to reconsider its findings. (Liam James Doyle for ║┌┴╧│╘╣╧═Ї News)
Unknown to Norton, Harbor aides had raised concerns about the other resident, who like Lynch was new to Harbor CrossingтАЩs memory unit, according to a . Diagnosed with AlzheimerтАЩs, severe dementia with agitation, depression, and anxiety, the woman was confused, had difficulty communicating her needs, and hit aides.
Aides repeatedly reported that the woman had тАЬongoing aggression, entered other residentsтАЩ apartments, invaded othersтАЩ personal space, and was difficult to redirect,тАЭ the health report said. They said medications had been ineffective and pressed for new ones. The report said one nurse told the womanтАЩs doctor it was тАЬonly a matter of time beforeтАЭ she тАЬhurts another resident.тАЭ
Captured on Camera
On the last day of September, she entered LynchтАЩs room and resisted leaving, the state report said. The next morning, she reappeared. Video of the incident was described in the police and state reports and reviewed by ║┌┴╧│╘╣╧═Ї News. It shows Lynch guided the woman out and appeared to attempt to lock the door, but the woman opened it and returned once more.
The woman declared it was her house, went into LynchтАЩs bathroom, used the toilet, and then returned to the room Lynch was in. Lynch can be seen repeatedly pressing the alert pendant around her neck to signal nurses for help.
The video shows the woman was almost out of her apartment door when she attempted to touch an object near the door. Lynch put her hands up to block her. The woman slapped at her hands and said, тАЬIтАЩm going to kill you if you donтАЩt quit it.тАЭ She pushed Lynch, who fell, her head hitting the floor and blood seeping out.
Aides arrived 13 minutes after she had initially pressed her pendant, the state report said. Lynch suffered a brain hemorrhage and fractures to her eye socket and ribs, according to the state report. She died in the hospital five days later at age 96; the medical examinerтАЩs office declared it a homicide.
Norton said her mother was kind and pleasant and never combative. тАЬMy mom deserved better than what they gave her,тАЭ she said.
Gladys Lynch was a department store accountant and raised three daughters before developing dementia. Here her daughter Rebecca Norton shows a collection of LynchтАЩs personal letters and photographs at NortonтАЩs home in Hugo, Minnesota. (Liam James Doyle for ║┌┴╧│╘╣╧═Ї News)
Prosecutors declined to bring charges, according to the police report. The Harbor Crossing was responsible for neglect because it was aware the woman тАЬexhibited violent and aggressive behaviorsтАЭ and yet had failed to put in place effective interventions. Harbor Crossing has requested the state reconsider its findings.
In June, Suzanne Scheller, the attorney for LynchтАЩs family, filed a wrongful death lawsuit against Presbyterian Homes, which owns Harbor Crossing.
Presbyterian said in a statement: тАЬWe are deeply saddened by the loss of Ms. Lynch, and our thoughts remain with her family and all those impacted.тАЭ It declined to comment further on the incident or the lawsuit.
Before Gladys LynchтАЩs death, employees at the memory care unit at Harbor Crossing in White Bear Lake, Minnesota, struggled to keep the resident who fatally assaulted her from behaving aggressively and wandering into other residentsтАЩ rooms, a state report found. Harbor Crossing has asked the state to reconsider its findings of negligence. (Liam James Doyle for ║┌┴╧│╘╣╧═Ї News)
Preventive Tactics
Geriatricians, researchers, and resident advocates say long-term care homes should to reduce the risk of altercations, including closer supervision of residents at high risk, relocating them closer to nursing stations, separating residents with repeated conflicts, and adjusting roommate assignments or seating in shared spaces.
Each resident should have a care plan, and homes should train staff to be alert to a residentтАЩs triggers and intervene quickly, dementia specialists say. Organized activities are essential to keep residents occupied and engaged. Antipsychotics and other psychotropic medications are often prescribed, but they can increase the risk of falls, strokes, and .
An aide can be assigned to watch a particularly challenging resident one-on-one, but many places lack enough staff for protracted, dedicated supervision. Some assisted living facilities will tell a residentтАЩs family they must hire a personal aide, who can cost thousands of dollars extra each month. In extreme situations, facilities might send a resident to an emergency room for evaluation or to a psychiatric hospital, or .
Camille Russell, who served as KansasтАЩ long-term care ombudsman until 2024, said she observed nurses and aides were often тАЬwoefully undertrainedтАЭ in basic elements of dementia care.
тАЬWeтАЩve gotten too far away from making decisions that are caring decisions,тАЭ Russell said. тАЬThere has to be a balance, and the balance has gotten too far to the profit side.тАЭ
A Debilitating Kick
Many physical altercations between residents result in a scratch or a bruise, but nonfatal scraps can leave permanent damage on deeply frail residents.
Linda TwiddyтАЩs first weeks in a Chesapeake, Virginia, memory care unit in August 2024 were happy, her daughter, Barbara Howerin, said in a May interview. Twiddy, a former church secretary with vascular dementia, sang along with a visiting church choir, decorated pumpkins, and visited a cat cafe. The facility, The Vero at Chesapeake, charged Twiddy a one-time $6,825 move-in fee and monthly charges of $7,475, according to the lease.
Seven weeks after Twiddy started living there, a nurse called Howerin. She told her that her mother had been kicked in an altercation with another resident and was being sent to the hospital.
When Howerin arrived at the hospital, she was shocked by the extent of the injury. тАЬIt was like 10 inches long by 6 inches wide, the whole front of her shin,тАЭ she said. тАЬThe calf was just like dangling down.тАЭ
According to an internal facility incident report the family obtained, an aide heard Twiddy scream for help and raced over to see a male resident with dementia trying to hit Twiddy as she sat on the floor in тАЬa pool of blood.тАЭ The report said, тАЬLinda was screaming get him away from me, he pushed and kicked me.тАЭ
The man had prior episodes of aggression, according to documents TwiddyтАЩs family obtained in a lawsuit they brought against The Vero in Chesapeake Circuit Court. At his previous facility, a progress note from 2023 stated, he was тАЬbecoming very aggressive in tone and actions to residents and staff.тАЭ He тАЬgrabbed another resident by the wrists and pushed her,тАЭ according to the note. He was sent to an emergency room for evaluation of agitation, according to a hospital report. It did not make clear whether he was discharged back to the facility or elsewhere.
Agitation Tied to Pain
The male residentтАЩs medical records at The Vero said he was diagnosed with late-onset AlzheimerтАЩs disease, agitation, and anxiety, according to his doctorтАЩs deposition. He had chronic pain in his back and trouble sleeping. He could answer simple yes-or-no questions but had trouble providing more extensive answers and couldnтАЩt communicate that he was in pain, she testified. His behavioral changes usually occurred when he had a urinary tract infection, the doctor said.
When he was agitated, aides could sometimes calm him by turning on the television so he could watch his beloved New England Patriots, one aide testified in a deposition. A former aide said she tried to avoid dealing with him altogether. тАЬIf you go up to him and he was agitated, heтАЩd reach out to try to grab you,тАЭ she testified. тАЬIf he had that cane, he would swing that cane or he would punch at you.тАЭ
In a court filing, The Vero denied allegations by TwiddyтАЩs family that it should have protected residents from him. The filing said The Vero complied with all standards of care and that any injuries Twiddy sustained тАЬwere caused by her own negligenceтАЭ or acts of others.
In their investigation of the incident, Virginia regulators alleged The Vero had for the health, safety, and well-being of its residents. The inspection report said The Vero pledged to appropriately staff the memory care unit based on the number of residents and to ensure someone completed rounds at least every two hours during sleeping hours.
Twiddy underwent three surgeries at the hospital for her leg, including a skin graft, then spent a month in rehabilitation. тАЬShe was never able to walk again,тАЭ her son, Doug Twiddy, said in a May interview.
The family moved Linda Twiddy to a different memory care facility where the nursing station had a clear view of all the rooms. She lived there until her death earlier this year.
The lawsuit was settled on confidential terms in early June. Carlton Bennett, the familyтАЩs attorney, declined to comment. In an email, Lauren Rogers, a spokesperson for Sinceri Senior Living, which operates The Vero, said the company was pleased the legal case had been resolved but could not comment further, citing confidentiality and patient privacy.
тАЬThe Vero at Chesapeake is committed to providing a caring, supportive environment where resident health, safety, and well-being remain our highest priorities,тАЭ she said.
A History of Violence
After Attilio Cecchetto was fatally bludgeoned at Sunrise Post Acute, his adult children and their attorney, Jody Moore, discovered disturbing details about Sam Ato Timaloa. He had been imprisoned in 1999 after being convicted of raping an underage girl and sentenced in 2008 to 24 years in prison for attempted murder involving domestic violence, according to Riverside County court records. His public defender declined to comment.
CecchettoтАЩs sons, Moore, and her colleagues at Moore Hutchins Moore also learned more about the homeтАЩs owner, PACS Group, a publicly traded company with more than 300 long-term care facilities. Last year, PACS earned $191 million on revenue of $5.3 billion, according to its .
In the Cecchettos and their fatherтАЩs widow filed against PACS, they accused the companyтАЩs founders, Jason Murray and Mark Hancock, of draining resources from their nursing homes to pay for the chainтАЩs expansion and swell their personal wealth.
The two had earned more than $650 million through stock sales since taking the company public and bought two private luxury jets, according to the lawsuit and securities filings. PACS has also purchased corporate sponsorships for Utah sports teams even though it owns no nursing homes in the state, the lawsuit said.
Attilio Cecchetto was allegedly beaten by his roommate at a California nursing home. Police photographed CecchettoтАЩs bed after he was taken to a hospital. He died two days later. (Banning Police Department)
California regulators fined Sunrise $120,000 for Cecchetto and for not taking TimaloaтАЩs articulated dislike of noise into account when assigning rooms. Medicare issued its own $62,810 fine.
In responding to the CecchettosтАЩ lawsuit, PACS denied negligence for his death and alleged he тАЬfailed to exercise ordinary care on his own behalf for his own safety.тАЭ It has sued to overturn the $120,000 state fine, saying it was issued too late and that Sunrise тАЬdid what might reasonably be expected of a long-term health care facility licensee acting under similar circumstancesтАЭ to comply with state rules.
The CecchettosтАЩ lawsuit asks for a judge to impose robust procedures PACS homes must follow for admissions, staff training, room changes, and the reporting of altercations between residents. The suit asks for a court-appointed monitor to oversee compliance. In its written statement to ║┌┴╧│╘╣╧═Ї News, PACS said тАЬimportant contextтАЭ would come out during the process and declined further comment.
In an interview, CecchettoтАЩs three sons, Dino, Gino, and Marco Cecchetto, described their fatherтАЩs life. He spent his childhood on a farm in Italy, growing up under Benito Mussolini. After World War II he moved to Canada, where he learned to tile and lay marble and terrazzo, a decorative flooring material made of chips of stone, glass, or other materials embedded in cement or resin. He relocated to California in the early 1960s, became naturalized, and worked as a tile journeyman and a contractor for decades.
тАЬWe donтАЩt want this to happen to somebody again,тАЭ Gino Cecchetto said. тАЬWith the life he led, he deserved a quiet, dignified death. Instead, he ended his life in pain and fear.тАЭ
Data Methodology
║┌┴╧│╘╣╧═Ї NewsтАЩ analysis of federal nursing home inspection reports focused on citations for violations of stating that each resident has the right to be free of abuse, neglect, and exploitation.
The analysis looked at the most serious levels of citations, those in which inspectors determined that one or more residents had been harmed, or that the facilityтАЩs actions caused тАФ or were likely to place residents in immediate jeopardy of тАФ serious injury, harm, impairment, or death. We reviewed the reports since January 2024 and tallied those that explicitly described resident-to-resident altercations.
We conducted a more granular analysis of a subset of the inspection reports from January through March 2026 involving harm or immediate jeopardy. Each report was reviewed and categorized by the type of abuse, neglect, or exploitation.
Pregnant WomanтАЩs Roadside Death Triggers Push To Reopen Mississippi Delta Hospital
Pregnant WomanтАЩs Roadside Death Triggers Push To Reopen Mississippi Delta Hospital
The closure of Humphreys County Memorial Hospital in Belzoni, Mississippi, meant that the nearest hospital to Harmony Ball-Stribling during her 2021 medical emergency was 25 miles away. (Shenelle Ball-Green)
BELZONI, Miss. тАФ Harmony Ball-StriblingтАЩs path to pregnancy had been turbulent, from an endometriosis diagnosis to an arduous in vitro fertilization process and sky-high blood pressure. But as her due date approached in the summer of 2021, her health improved and those storm clouds seemed to scatter.
тАЬIt was just too perfect,тАЭ said her mother, Shenelle Ball-Green, of those calm, hot weeks.
Then, early on July 5, four days shy of her scheduled cesarean section, Ball-Stribling began experiencing complications from preeclampsia, a potentially life-threatening blood pressure disorder. Speeding up to 110 mph, her husband drove her to the nearest hospital 25 miles away from their home in Belzoni, a Mississippi Delta town of about 1,900 people.
Minutes before reaching the facility, Ball-Stribling suffered a seizure in the passenger seat. Her husband pulled her from the car and performed CPR on the side of the road. It was too late. She and the coupleтАЩs unborn daughter, Harper, died on the side of U.S. Route 49.
The tragedy might have had a different outcome if the hospital in Belzoni, a five-minute drive from Ball-Stribling’s home, hadnтАЩt closed 13 years ago. Today, Humphreys County has no hospital, no emergency room, no urgent care clinic, and no county health department. It is one of more than in the U.S. that have fully closed since 2005.
In Belzoni, self-proclaimed тАЬThe Heart of the Delta,тАЭ and its surrounding area, communities are close-knit, and HarmonyтАЩs story is well known. Now, her death has galvanized local and state leaders determined to bring a hospital back to the county that has suffered without one.
тАЬIt was a tremendous eye-opener for this community,тАЭ said state Rep. Timaka James-Jones, a Democrat who represents the district that includes Belzoni and is Ball-StriblingтАЩs aunt. тАЬIt brought to light how we are so without.тАЭ
Poverty often shapes the health disparities Humphreys County residents experience. Approximately under age 65 lack health insurance coverage, compared with about 1 in 11 people nationwide. Humphreys County also has the of any Mississippi county, reflecting the economic challenges many residents face. These disparities are evident in the countyтАЩs infant mortality rate, which is at roughly 15 deaths for every 1,000 births.
James-Jones has watched these circumstances influence the lives тАФ and deaths тАФ of her loved ones. She said she wants to see a hospital reestablished before her four-year term is up in early 2028.
But that may be easier said than done. In Belzoni, local leaders hoping to restore healthcare services face a tangled web of policy challenges that are especially demanding for a small town with limited resources. Its story reflects what many : Once a rural community loses a hospital, bringing it back can be nearly impossible.
Belzoni, Mississippi (Vickie D. King/Mississippi Today)
Humphreys CountyтАЩs Healthcare Losses
Humphreys County Memorial Hospital opened in Belzoni in 1951 as part of a nationwide hospital building boom fueled by a Truman-era law called the Hill-Burton Act. The legislation provided billions of dollars in grants and loans to build and modernize healthcare facilities. At the time, had no hospital. When the building boom began to subside by 1970, in Mississippi had at least one hospital.
But by the 2000s, many rural hospitals in the U.S. confronted financial difficulties. Low patient volumes, an increase in outpatient care, and meager revenues left many on precarious footing. Many had high rates of uninsured patients or those covered through government programs such as Medicaid, which typically reimburse providers at lower rates than commercial insurers.
Humphreys CountyтАЩs hospital was among those struggling facilities. It was burdened with , and county officials sold it in 2008 to a private company. It was renamed the PatientsтАЩ Choice Medical Center. The hospital shut down five years later after Ray Shoemaker, the companyтАЩs CEO, was convicted on healthcare fraud charges related to another hospital he owned.
тАЬI do hope they reopen,тАЭ Shoemaker wrote in a recent text message to Mississippi Today. тАЬThe community needs a hospital.тАЭ He said he stepped down from the company before going to prison in 2012.
Email Sign-Up
Subscribe to ║┌┴╧│╘╣╧═Ї News' free Morning Briefing.
In 2017, the University of Mississippi Medical Center partnered with the county supervisors and U.S. Rep. Bennie Thompson, a Democrat whose district includes Humphreys County, to secure a from the U.S. Department of Agriculture to open an after-hours acute care clinic in Belzoni. The clinic shut down in 2020, and UMMC officials declined to say why.
G.A. Carmichael Family Health Center, a Canton-based federally qualified health center with five other locations in Mississippi, took it over but did not maintain the extended hours, again leaving Humphreys County residents without after-hours care. Other public health services in the county have closed outright. Three years ago, the countyтАЩs health department stopped providing clinical services, said Greg Flynn, a spokesperson for the Mississippi State Department of Health. The county department closed entirely last year, citing staffing shortages and low patient volumes.
In the years since the hospital closed, the county has lost a fourth of its population, falling to 7,000 people, . James-Jones said she does not believe the community can experience growth until healthcare services are reestablished.
тАЬI donтАЩt know how I can see us growing any other way,тАЭ she said.
Shenelle Ball-Green lost her daughter, Harmony Ball-Stribling, and unborn grandchild in July 2021 during a medical emergency as Ball-Stribling was en route with her husband to the nearest hospital, 25 miles away. (Vickie D. King/Mississippi Today)
тАШSomethingтАЩs Way Better Than NothingтАЩ
Months after losing her daughter and unborn granddaughter, Ball-Green climbed the steps of the stately, tan, brick Humphreys County Courthouse to attend a crowded Board of Supervisors meeting.
She stood at the dais and urged the supervisors to reestablish emergency healthcare services in the county to protect other residents from the fates of her loved ones.
тАЬI wanted to let them know at any given moment that could be your child, your mother,тАЭ she said. тАЬWeтАЩre a small town. Everyone knows everyone.тАЭ
She remembered the disappointment she felt when the supervisors told her there was nothing they could do. But when the boardтАЩs makeup changed after the 2023 elections, she said, she saw these attitudes shift.
The Humphreys County Courthouse is located in Belzoni, Mississippi. (Vickie D. King/Mississippi Today)
Among the newly elected officials was Reggie Pinkston, who is now the president of the board and previously worked as an EMT when the hospital was open. His own family has suffered the consequences of limited healthcare access. A cousin living in Louise, a town about 20 miles south of Belzoni in the county, had a stroke in 2021 and waited an hour for an ambulance to arrive. She died two days later.
Pinkston said witnessing residentsтАЩ delays in care has made expanding access to healthcare services one of his priorities.
тАЬWeтАЩre losing too many people in our county because of lack of healthcare,тАЭ Pinkston said.
The board enlisted several consultants to develop a strategy for expanding healthcare access and identifying funding sources to support these efforts. In late 2025, Thompson secured for Humphreys County through the congressional Community Project Funding process, which allows lawmakers to request federal support for specific projects.
The funds will be used to expand services at G.A. CarmichaelтАЩs Belzoni location in a county-owned building on U.S. Route 49, Pinkston said. Expansion plans include extending its hours of operation overnight to 5 a.m., purchasing equipment, and a possible renovation of the facility. It could begin its expanded operations by September, said James Coleman Jr., the health centerтАЩs CEO.
Establishing an after-hours urgent care clinic is a starting point toward reestablishing emergency care services or a hospital, James-Jones said.
тАЬSomethingтАЩs way better than nothing,тАЭ she said.
Mississippi state Rep. Timaka James-Jones, a Democrat who represents the district that includes Belzoni, is one of the community leaders spearheading an effort to reestablish a hospital in Humphreys County. (Vickie D. King/Mississippi Today)
тАШNot for the Faint of HeartтАЩ
Despite that encouraging first step, Humphreys County faces steep obstacles to opening a hospital.
At the University of North Carolina-Chapel Hill, George Pink is a senior research fellow at the Cecil G. Sheps Center for Health Services Research and tracks rural hospital closures across the U.S. He said heтАЩs aware of only a few communities that have successfully reopened a hospital after it closed.
тАЬI can count that on one hand,тАЭ said Pink, who knows of roughly five such examples.
Communities face significant hurdles to reestablishing a hospital, including securing financing for construction or renovation, recruiting qualified staff, and covering substantial operating expenses during the licensing process before the facility can treat patients and generate revenue, said Brock Slabach, the National Rural Health AssociationтАЩs chief operations officer and a former rural hospital administrator in southwestern Mississippi.
тАЬReopening a hospital is not for the faint of heart,тАЭ Slabach said. тАЬOnce they close, itтАЩs very difficult to reopen them.тАЭ
To finance a potential hospital project in Humphreys County, local and state leaders said they plan to seek funding through the Rural Health Transformation Program, a federal initiative that will distribute $50 billion to states over five years. The federal government allocated Mississippi in December for the programтАЩs first year.
The program is meant to offset budget cuts passed into law last summer that could harm rural hospitals. RepublicansтАЩ One Big Beautiful Bill Act Medicaid spending by $911 billion over 10 years and increase the number of uninsured people by 10 million, according to Congressional Budget Office estimates. Mississippi hospitals are beginning in 2029, according to Cindy Bradshaw, executive director of the Mississippi Division of Medicaid.
But , the programтАЩs funding cannot be used for construction or major building expansions. Officials said the county will instead consider applying for funds through the program to support the recruitment of healthcare professionals.
The federal Rural Emergency Hospital designation is another way rural communities can keep emergency and outpatient services. Hospitals in that program receive over $3 million annually from the federal government and a higher Medicare reimbursement rate, but they .
Research by PinkтАЩs team shows that many hospitals that converted to the model, which was established in 2023, saw an .
But thereтАЩs a catch. To receive the designation, a hospital must have been open in 2020, making Humphreys County ineligible. MississippiтАЩs junior U.S. senator, Republican Cindy Hyde-Smith, introduced legislation in 2024 to to 2014, a threshold that would have still excluded Humphreys County.
James-Jones said county leaders have urged Hyde-Smith to amend the proposed legislation so Humphreys County could qualify. Hyde-Smith did not respond to a request for comment for this article.
Belzoni, Mississippi, is self-proclaimed тАЬThe Heart of the Delta.тАЭ (Vickie D. King/Mississippi Today)
For county leaders, the path to widening healthcare access means navigating a thicket of state and federal policies, funding streams, and regulatory hurdles.
Some recent state-level policy changes have created opportunities for healthcare expansion in Humphreys County. In March, Republican Gov. Tate Reeves exempting Humphreys County from MississippiтАЩs certificate of need requirements, which are meant to prevent unnecessary healthcare expansions.
The exemption could make the county more attractive to prospective healthcare providers. But the financial challenges that contributed to the closure of PatientsтАЩ Choice Medical Center in 2013 remain, and Mississippi lawmakers have continued to reject Medicaid expansion, limiting a potential source of reimbursement for rural hospitals and clinics.
Industry officials expect hospitalsтАЩ financial pressures to intensify as Medicaid funding cuts take effect. The latest challenge is predicting how these cuts will affect the bottom lines of these facilities and whether additional cuts will come in the future, said Richard Roberson, president and CEO of the Mississippi Hospital Association.
тАЬIf someoneтАЩs trying to run a business, theyтАЩve got to be able to know what those numbers look like,тАЭ Roberson said. тАЬAnd itтАЩs really hard to try to project that out right now.тАЭ
The G.A. Carmichael Family Health Center, a federally qualified health center with five other locations in Mississippi, took over an acute care clinic in Belzoni, which shut down in 2020. (Vickie D. King/Mississippi Today)
тАШNow I UnderstandтАЩ
For Ball-Green, giving in to these obstacles would be a disservice to the Humphreys County residents who face health emergencies similar to the one her daughter experienced.
It has been five years since the funeral, but Ball-Green remembers it clearly. The day was stormy, but attendees brightened the gathering by wearing yellow, Ball-StriblingтАЩs favorite color.
As friends and family gathered to pay their respects, her mother thought back on a relativeтАЩs funeral four months earlier. At that service, Ball-Stribling sang the gospel classic You Are My Strength to a roomful of mourners.
тАЬShe was singing, and she looked at me,тАЭ Ball-Green said, describing a peaceful but eerie expression on her daughterтАЩs face in that moment тАФ a sign of something to come, though she didnтАЩt yet know what. тАЬShe turned around, and it was just that look, you know?тАЭ
Months later, as she sat at her daughterтАЩs funeral, she began to interpret the foreboding glance differently. She came to believe it was a sign that Ball-StriblingтАЩs gift for helping others by sharing her story would not end with her death.
That purpose had taken shape years earlier in her work as a teacher and continued as she shared about her fertility struggles and IVF journey in the final months of her life. Ball-Green said the community became deeply invested in her and HarperтАЩs story.
In the years since, this gift has endured, she said. Ball-StriblingтАЩs story has continued to resonate throughout Humphreys County, serving as a reminder of what residents stand to lose if they do not reopen the hospital.
тАЬI think back on when she looked back at me,тАЭ Ball-Green said. тАЬNow I understand.тАЭ
Journalists Dig Into HHS’ Covid Injury List, ACA Sign-Ups, and Telehealth
Journalists Dig Into HHS’ Covid Injury List, ACA Sign-Ups, and Telehealth
July 18, 2026
C├йline Gounder, ║┌┴╧│╘╣╧═Ї NewsтАЩ editor-at-large for public health, discussed the Department of Health and Human Services’ plan to offer compensation for automatic covid vaccine injuries and the drop in enrollment in Affordable Care Act health plans on CBS’ The Takeout With Major Garrett on July 10 and 9, respectively.
.
.
║┌┴╧│╘╣╧═Ї News Southern correspondent Sam Whitehead discussed abortion telehealth on WUGA’s The Georgia Health Report on July 10.
Big Employers Increasingly in Hot Seat as Medicaid Work Requirements Loom┬а
July 17, 2026
As they prepare to enforce new federal rules requiring millions of low-income people to prove they are working to keep their Medicaid coverage, some states want to spotlight businesses that rely on the government program to provide their employees with health insurance.
California lawmakers seek to bring back a law that requires the state to publicly list those companies that employ 100 or more people and have workers enrolled in Medi-Cal, the stateтАЩs Medicaid program. Nevada has had a similar law in place since 2017.
тАЬItтАЩs a basic principle that taxpayers deserve transparency about which large employers are shifting their healthcare costs onto the public,тАЭ said California state Sen. Lola Smallwood-Cuevas, a Democrat and the billтАЩs sponsor.
Some states are going further than simply naming and shaming companies. Democratic New Jersey Gov. Mikie Sherrill signed a bill in June to fine businesses with at least 50 workers on Medicaid from $325 to $725 a year for each employee and dependent enrolled.
Similar proposals stalled in Washington state and Colorado this year.
Email Sign-Up
Subscribe to ║┌┴╧│╘╣╧═Ї News' free weekly newsletter, "The Week in Brief."
A January deadline looms for states to enforce the new Medicaid work requirements under the One Big Beautiful Bill Act, which President Donald Trump signed last summer. For enrollees to keep their coverage after January, theyтАЩll need to prove they are working, volunteering, or going to school at least 80 hours per month. This applies to nondisabled enrollees ages 19 to 64 in most states.
The change carries a significant administrative and financial burden for states that must implement it along with other adjustments to the joint state-federal program.
One health policy researcher said the push to identify businesses with employees on Medicaid highlights the lack of affordable healthcare options available to low-wage workers.
тАЬThereтАЩs a whole set of people who are working тАФ they may not satisfy the work requirement provisions, they may not get the exemption that theyтАЩre qualified for, and they donтАЩt have access to that employer-sponsored insurance either,тАЭ said Edwin Park, a research professor at the Center for Children and Families at Georgetown University.
Nearly 5 million of the more than 14 million California residents on Medi-Cal will be subject to work requirements.
Compounded by changes to the federal Supplemental Nutrition Assistance Program, or SNAP, people may need to choose between paying for medicine or paying for rent when they lose food and health benefits, Smallwood-Cuevas said.
тАЬWeтАЩre going to see more people in their cars, more people on the street, and a lot more people in the emergency room,тАЭ she said. тАЬThat is dangerous for all of California.тАЭ
With the federal Medicaid work requirements looming in January, Democrats are considering state legislation to call out big companies that employ workers enrolled in the safety net health program. Business giants such as Amazon and Walmart said the figures are misleading.
In this тАЬHow Would You Fix It?тАЭ interview, Julie Rovner, ║┌┴╧│╘╣╧═Ї NewsтАЩ chief Washington correspondent and host of the What the Health? podcast, sat down with Elizabeth Mitchell, the president and CEO of the Purchaser Business Group on Health, which represents many large employers and other institutional buyers of healthcare coverage.
Mitchell noted that employers, which offer coverage to more than 160 million Americans, are a big player in the nationтАЩs healthcare system тАФ a role they came into because of тАЬan accident of history,тАЭ she said.
тАЬThey werenтАЩt looking to get into the healthcare business,тАЭ she continued, but тАЬthey were looking for alternatives to wages when there were limits on what they could offer, and they started with what was a pretty inexpensive offering тАФ helping pay for hospital care тАФ and that has now grown to be the second-largest line item in their budgets after payroll.тАЭ
Rovner and Mitchell discussed the fact that while large employers do have market power, the rest of the healthcare system banded together in response.
тАЬThereтАЩs been this arms race of consolidation, meaning that even the largest employers in the world are smaller and donтАЩt have the leverage many times,тАЭ Mitchell said.
Asked to identify the systemic changes large employers would like to see, Mitchell pointed to boosting primary care and referring patients to high-quality specialists. She said changes to business policies тАФ in particular, banning anti-competitive practices and increasing price transparency тАФ would help, too.
тАЬWe have a very real affordability crisis,тАЭ she said.
An abbreviated version of this interview aired July 16 during Episode 455 of What the Health? From ║┌┴╧│╘╣╧═Ї News: тАЬStates Start Their Medicaid Cuts.тАЭ
Insurers Hedge on Trump-Backed Pledge To Improve Denials Process
Health and Human Services Secretary Robert F. Kennedy Jr., joined by officials including Centers for Medicare & Medicaid Services Administrator Mehmet Oz (second from left), speaks at a June 2025 news conference to announce a plan aimed at improving health insurance companies' prior authorization processes for consumers. (Saul Loeb/AFP via Getty Images)
One year after the Trump administration announced that dozens of health insurers had signed promising to reduce barriers to doctor-recommended care, some insurers now say they wonтАЩt implement all the promised initiatives.
Meanwhile, patients, their advocates, and clinicians say little has improved.
тАЬIt has never been this bad for patients,тАЭ said U.S. Rep. Greg Murphy (R-N.C.), a physician who co-chairs the GOP Doctors Caucus.
The overarching intent of the June 2025 pledge was to improve a controversial process called prior authorization, which regularly requires patients or someone on their medical team to seek approval from insurers before proceeding with treatment.
According to AHIP, the health insurance industry trade group, health plans have eliminated 6.5 million prior authorizations for patients тАФ equal to an 11% reduction тАФ since the announcement.
But critics remain skeptical. Sally Nix, a patient advocate who has a chronic disease, described the voluntary pledge as тАЬperformative.тАЭ And Murphy, who participated in the news conference with Health and Human Services Secretary Robert F. Kennedy Jr. announcing the pledge last year, said it has тАЬno teeth.тАЭ
Voluntary insurer pledges rarely make things better for patients, said , a research professor at the Center on Health Insurance Reforms at Georgetown University.
тАЬIn the absence of clear rules, policies, standards, and mandates,тАЭ she said, insurance companies are тАЬgoing to do what makes sense for them to do financially.тАЭ
The Department of Health and Human Services did not respond to questions for this report. It isnтАЩt clear how, or whether, the Trump administration is holding insurers accountable.
Email Sign-Up
Subscribe to ║┌┴╧│╘╣╧═Ї News' free weekly newsletter, "The Week in Brief."
тАШZero FaithтАЩ
Prior authorization тАФ sometimes called preauthorization or precertification тАФ has been around for decades. The insurance industry has long argued that the practice, which varies by company, helps control costs, reduces waste and fraud, and prevents potential harm to patients. ItтАЩs regularly invoked for a huge swath of services, ranging from low-cost urgent care to expensive cancer treatment.
тАЬPrior authorization is a vital patient safeguard,тАЭ said Chris Bond, a spokesperson for AHIP.
The 2024 killing of UnitedHealthcare CEO Brian Thompson sparked a national groundswell of anger about insurance denials, with patients and doctors becoming increasingly vocal about the tactics they say insurance companies use to boost profits at the expense of care.
Prior authorization reform is one of the rare healthcare issues Democrats and Republicans tend to agree on. On July 15, the House Ways and Means Committee unanimously that would force Medicare Advantage plans to provide to the federal government a list of all items and services that are subject to prior authorization, and to report data about denials and grievances, among other requirements.
Last yearтАЩs industry pledge was organized as a direct response to public anger, Mehmet Oz, administrator of the Centers for Medicare & Medicaid Services, said when it was announced. тАЬThereтАЩs violence in the streets over these issues,тАЭ he said.
тАЬAmericans are upset about it,тАЭ Oz said, later adding, тАЬIтАЩm looking forward to seeing the results.тАЭ
Mike Gartner, founder of Health Access Innovation, an organization that helps patients overturn insurance denials, said he doubts that insurance companies are changing their policies in meaningful ways. The 11% reduction in prior authorization cited by AHIP тАЬhides a lot of nuance,тАЭ Gartner said.
Patients who need the costliest services, such as cancer treatment, are still being disproportionately denied access to doctor-recommended care, he said.
AHIP said its data included reductions in prior authorization for medical services, not prescription medicines. The trade group didnтАЩt provide details explaining which services have been dropped from prior authorization or how those reductions differ across individual insurers.
Last year, Oz said the federal government would be тАЬevaluating progressтАЭ toward the pledge and тАЬdriving accountability,тАЭ and he foreshadowed тАЬpublic dashboards.тАЭ But no such dashboards exist, and federal officials did not respond to questions about how theyтАЩre holding companies accountable.
Murphy, the North Carolina congressman, said he has тАЬzero faithтАЭ in the industry policing itself.
He didnтАЩt believe insurance companies then, he said, тАЬand I donтАЩt believe them now.тАЭ
тАШAt WarтАЩ With an Insurer
In February, days after Betsy Adler and Justin YoungтАЩs daughter Coco was born with a serious heart defect, the Stillwater, Minnesota, family received paperwork showing they were racking up out-of-network costs.
During AdlerтАЩs pregnancy, the family had switched insurers, , which is based in Minnetonka, Minnesota, and one of that initially signed the industry pledge. Adler said sheтАЩd checked with her employerтАЩs human resources department and on MedicaтАЩs website to make sure her maternal-fetal specialists and hospital were in-network before their new health plan went into effect earlier this year.
But then, the insurance company started processing some claims as out-of-network. By mid-March, the family had accrued more than $4,000 in out-of-network charges, on top of more than $3,000 for in-network bills. And the bills kept coming.
Shortly after Betsy AdlerтАЩs daughter Coco was born with a serious heart defect, she started receiving estimates showing her family could owe thousands of dollars in outтАУof-network costs. (Justin Young)
Adler had switched insurers to Medica during her pregnancy and said she was assured that her care would be covered at in-network rates. (Justin Young)
When Adler, a psychotherapist, called to figure out what was going on, she said, an insurance company representative said she hadnтАЩt submitted a referral from her primary care provider beforehand. Attempts to fix the problem went nowhere. At one point, Adler said, Medica required her to visit a clinic sheтАЩd never been to before to obtain a referral. But she said a Medica representative told her the referral was never received, because the insurerтАЩs fax machine was down.
тАЬI have a critically ill child,тАЭ Adler remembered thinking shortly after Coco was discharged from the cardiovascular intensive care unit. тАЬI can either spend my emotional energy at war with Medica, or I can let it go and just enjoy my time with my daughter.тАЭ
Medica spokesperson Greg Bury said he wouldnтАЩt discuss the case, citing patient privacy rules. In an emailed statement, he wrote the company is тАЬcommitted to working with her to ensure she understands what is covered under her benefits and our responsibilities.тАЭ
One of six specific promises all insurers made when they signed the pledge was to honor a 90-day grace period when patients switch insurance plans, starting Jan. 1 of this year. Often called тАЬcontinuity of care,тАЭ this grace period allows patients to temporarily continue receiving services and medications that were authorized under a previous insurer.
But that applies only in some circumstances, GeorgetownтАЩs Corlette said. The wording of the pledge suggests that insurance companies arenтАЩt obligated to honor another companyтАЩs network parameters. When Adler and Young switched insurers, for example, Medica was not obligated to cover the cost of out-of-network providers as if they were in-network, even though they were in-network under the familyтАЩs old plan.
Adler and Young switched insurance companies again when Coco was a month old, to avoid accruing more out-of-network costs.
Denial After Approval
Sally Nix with her service dog, Jon Snow, at home in Statesville, North Carolina. Nix, a patient advocate, recently had her health insurer process, then later deny, a claim for injections to relieve her chronic nerve pain. SheтАЩs skeptical about industry promises to reform the health insurance denial process. (Logan Cyrus for ║┌┴╧│╘╣╧═Ї News)
The percentages cited by AHIP donтАЩt tell the whole story, said Nix, the patient advocate. Insurers are тАЬnot including the data for the loopholes they create,тАЭ she said.
For example, nothing in the pledge prevents insurance companies from retroactively denying payment, even when care is preapproved. тАЬPatients are going to see a lot more retroactive denials,тАЭ said Nix, who recently had her insurer process, then later deny, a claim for injections to relieve her nerve pain.
Something similar recently happened to Jocelyn Austin, 49, of Amherst, New York. Over the course of nearly 20 years, she developed an addiction to sleeping and anxiety pills prescribed to her by a doctor. Last year, she spent weeks at an inpatient treatment center for substance abuse. Her insurer, Independent Health, had approved the admission. Austin said she has been substance-free since her discharge.
But the facility sent her a bill for more than $12,000 in December showing her insurer had not paid for the treatment she received, according to documents Austin shared with ║┌┴╧│╘╣╧═Ї News. This was in addition to the $10,000 she paid at the beginning of her treatment to satisfy her out-of-network deductible. The approval letters from Independent Health had specified that тАЬauthorization is not a guarantee of claim payment.тАЭ
Frank Sava, a spokesperson for Independent Health, said a denial was issued and upheld in this case because the services provided тАЬwere inconsistent with the care that was authorizedтАЭ and тАЬthe medical record did not sufficiently support what was billed.тАЭ He said those findings were reviewed and confirmed by an outside consultant.
An explanation of benefits issued by the insurer last summer indicated the тАЬprovider,тАЭ not the patient, was responsible for the cost of her treatment. And yet the treatment facility has continued to pressure her for payment, she said.
Austin, who has not paid her outstanding bill, said insurance companies тАЬshould be held accountable.тАЭ
тАШSignificant Work AheadтАЩ
Another one of the six commitments insurers made last year was to adopt new technology that would standardize the electronic submission of prior authorization requests. During the news conference announcing the pledge last summer, Chris Klomp, the director of Medicare and a deputy CMS administrator, said more than 50% of prior authorizations are still paper-based and processed by phone or fax machine.
In April, AHIP related to that technology initiative, explaining that participating insurers would adopt the new standards on a rolling basis. Health insurers agreed to implement the pledgeтАЩs various commitments by predetermined deadlines, and this initiative is scheduled to be operational by Jan. 1, 2027. But eight insurers that initially signed the pledge last year didnтАЩt sign the technology update when it was announced in April, AHIP told ║┌┴╧│╘╣╧═Ї News.
Those insurers are Alignment Health Plan, EmblemHealth, HealthFirst, Independent Health, Medica, MVP Health Care, Point32Health, and SummaCare. Their beneficiaries span the country, from California to New York. None of those eight insurers agreed to interviews for this report, but most sent ║┌┴╧│╘╣╧═Ї News emailed statements indicating that they remain committed to prior authorization reform.
AHIPтАЩs approach to continuity of care тАЬwould have required the transfer of confidential member health information through a non-standardized process involving third-party participation,тАЭ wrote Jerry Slowey, a spokesperson for , which offers Medicare Advantage policies in Arizona, California, Nevada, North Carolina, and Texas. тАЬWe do not believe that level of data sharing was contemplated in the original commitment.тАЭ
Bury, the spokesperson for Medica, which covers beneficiaries in Iowa, Kansas, Minnesota, Missouri, Nebraska, North Dakota, Oklahoma, South Dakota, and Wisconsin, said the company тАЬsupports the goal of these standardization efforts.тАЭ But the April update тАЬraised a significant technical and operational hurdle that we are not able to commit to at this time,тАЭ he said.
Alex Gomez, a spokesperson for EmblemHealth, said in late June the company тАЬwill sign onto the commitmentтАЭ after ║┌┴╧│╘╣╧═Ї News posed questions about why it had not endorsed the April update.
тАЬWe anticipate more plans will be added over the coming months,тАЭ said Bond, the AHIP spokesperson. Health plans are тАЬworking continuously to implement their commitments to simplify and improve the experience.тАЭ He acknowledged that тАЬthere is still significant work ahead.тАЭ
The original pledge also included a promise that insurance companies would enhance transparency and use тАЬclear, easy-to-understand explanationsтАЭ when communicating to patients тАФ something they were already supposed to be doing under the Affordable Care Act.
Yet companies still regularly neglect to explain why care has been denied, and their communications often contain тАЬinconsistent and contradictory information,тАЭ said Gartner, of Health Access Innovation. He and Murphy also said they suspect insurance companies are increasingly using artificial intelligence to generate denials.
тАЬThey craft the pathways to basically deny things immediately with the hope that people will give up,тАЭ Murphy said.
The congressman said he wishes President Donald Trump would sign executive orders addressing some of these issues. тАЬThe problem is the insurance industry is the strongest lobby in this town.тАЭ
Do you have an experience with prior authorization youтАЩd like to share? to tell ║┌┴╧│╘╣╧═Ї News your story.
TrumpтАЩs CDC Nominee Praises Vaccines, Without Vowing Independence From Kennedy
TrumpтАЩs CDC Nominee Praises Vaccines, Without Vowing Independence From Kennedy
Erica Schwartz, President Donald TrumpтАЩs pick to lead the Centers for Disease Control and Prevention, appears before the Senate Health, Education, Labor and Pensions Committee on July 15. (Eric Harkleroad/║┌┴╧│╘╣╧═Ї News)
Erica Schwartz, President Donald Trump’s nominee to lead the Centers for Disease Control and Prevention, expressed support for vaccines тАФ including mRNA-based covid shots тАФ in a Senate hearing on Wednesday, though she didnтАЩt dispel concerns the agency has lost any independence from the White House.
тАЬI have been vaccinating people throughout my entire career in uniformed services. I believe in vaccines,тАЭ Schwartz said at the hearing. тАЬI do believe that mRNA technology is safe and effective.тАЭ
Her position contrasts with that of Health and Human Services Secretary Robert F. Kennedy Jr., who ousted TrumpтАЩs previous CDC director, Susan Monarez, after she sparred with him over vaccines. Kennedy, a longtime anti-vaccine activist, has baselessly called mRNA vaccines the deadliest ever made.
Schwartz тАЬhas dedicated her career to protecting the health of the American people.тАЭ Emily Hilliard, an HHS spokesperson, said in an emailed statement. тАЬThe president nominated her because of that exemplary record, and Secretary Kennedy looks forward to working with her to advance the AdministrationтАЩs public health priorities.тАЭ
The CDC has had a Senate-confirmed leader for only about one month during TrumpтАЩs second term, and the agency has been roiled over the administrationтАЩs cuts to public health funding, firings of scientists and other career employees, and efforts to scale back childhood vaccines and access to covid shots.
Schwartz, who was deputy surgeon general in TrumpтАЩs first administration and is a former chief medical officer for the Coast Guard, has support in the public health community, where itтАЩs hoped she can restore credibility at the agency she would lead.
тАЬI will follow the science wherever it leads,тАЭ Schwartz told senators. тАЬMy first priority will be restoring trust in public health institutions.тАЭ
Email Sign-Up
Subscribe to ║┌┴╧│╘╣╧═Ї News' free Morning Briefing.
Democrats and some Republicans have expressed doubt that Schwartz will maintain any more independence from Kennedy than Monarez, who has said she was fired in August after refusing to sign off on changes Kennedy demanded to vaccine recommendations and personnel cuts. In a released by Sen. Bernie Sanders (I-Vt.), it was revealed Kennedy had pressured Monarez to change CDC guidance regarding the universal childhood flu vaccine.
Monarez тАЬrefused to act as a rubber stamp for Secretary Kennedy’s very dangerous agenda,тАЭ Sanders said July 15 at the Health, Education, Labor and Pensions CommitteeтАЩs confirmation hearing for Schwartz. тАЬFrankly, she stood up for protecting the well-being of the American people.тАЭ
The chairman of the HELP Committee, Sen. Bill Cassidy (R-La.), pressed Schwartz on whether she would push back against rhetoric or policies not based in science.
тАЬWe need unbiased leaders who make decisions based upon science, not politics or ideology,тАЭ Cassidy said. тАЬThis is not a theoretical.тАЭ
Cassidy, a physician, has also quarreled with Kennedy over vaccines. He lost a Republican primary for reelection in May after Trump endorsed one of his opponents. Despite his rupture with the White House, Schwartz almost certainly needs CassidyтАЩs support to win confirmation. That requires publicly committing to support vaccination and mainstream science.
Schwartz told the committee she would тАЬnever compromiseтАЭ on science.
тАЬThe president would never ask me to not follow the law,тАЭ she said. тАЬBut I will always follow the law.тАЭ
Sen. Bill Cassidy (R-La.), chairman of the Health, Education, Labor and Pensions Committee, questioned Schwartz on her support of vaccines and her willingness to push back against her would-be boss, health secretary Robert F. Kennedy Jr. (Eric Harkleroad/║┌┴╧│╘╣╧═Ї News)
Many Democrats on the committee raised concerns about the administrationтАЩs politicization of public health. Sen. Tammy Baldwin (D-Wis.) asked about the тАЬpolitical scrubbingтАЭ of research grants. Trump officials have canceled many research grants under the CDC and the National Institutes of Health for political reasons, including targeting diversity, equity, and inclusion efforts.
тАЬRestoring trust to the CDC is my No. 1 priority,тАЭ Schwartz said. тАЬScientific integrity is core.тАЭ
The American Public Health Association’s CEO, Georges Benjamin, , saying she тАЬpossesses the medical background and public health knowledge to understand that the Centers for Disease Control and Prevention must be guided by evidence-based science.тАЭ
The APHA has fought many of TrumpтАЩs initiatives on public health. After MonarezтАЩs resignation, the organization titled тАЬKennedyтАЩs attack on public health must be stopped.тАЭ
Schwartz told the committee that if she is confirmed, she is committed to “radical transparency” and modernization.
Schwartz expressed support for one Kennedy initiative: She told senators she believes nutrition education and physical fitness assessments are important.
“I am all in on the Make America Healthy Again agenda,” she said.
At the July 15 hearing, Schwartz faced questioning alongside Trump’s pick for HHS assistant secretary for preparedness and response, Sean Kaufman.
Schwartz testifies alongside President Donald Trump’s pick for the role of Health and Human Services assistant secretary for preparedness and response, Sean Kaufman. (Eric Harkleroad/║┌┴╧│╘╣╧═Ї News)
Cassidy called out Kaufman for past comments casting doubt on the efficacy of vaccines. The senator raised his voice as he accused Kaufman of spreading тАЬthose damn lies.тАЭ
Kaufman was conciliatory. тАЬLet me be clear: Vaccines save lives,тАЭ he said. тАЬThey are safe and effective.тАЭ
If confirmed by the Senate, Schwartz will replace Jay Bhattacharya, who is performing the duties of CDC director but is not officially the acting director. Bhattacharya is also the director of the NIH.
Readers Share Personal Insights on Deadly Denials and Pregnancy Centers
My husband, Kenney, had chronic obstructive pulmonary disease. On June 7, he fatally shot himself after a COPD exacerbation event.
His pulmonologist had prescribed two new nebulizer prescriptions on June 2. One was a specialty medication that would come directly from the drug company. A couple of days later, we called Walgreens to see why the other one hadnтАЩt been filled. Turns out it required prior authorization.
Why the doctor who prescribed it needed to tell his health insurer that he really did think his patient needed it, I will never understand. The pharmacist said she would send the request to the doctor. And why she hadnтАЩt already done that, again, I do not understand. By June 7, of course, it still wasnтАЩt filled.
That day, a Sunday, Kenney experienced the flare-up when I was out mowing the yard. How terrifying it must have been for him to be unable to breathe and me not being there at least to hold his hand. That night he killed himself, leaving a note saying that he hated to leave me but that he couldnтАЩt keep living like that тАФ with the constant anxiety of not knowing when he wouldnтАЩt be able to draw a breath.
Not long ago, a тАЬwelcomeтАЭ packet came in the mail about the other nebulizer treatment тАФ 25 days after it had been prescribed.
Admittedly, my husbandтАЩs health was not great. He did have COPD, but we still went out to eat once in a while, and he didnтАЩt have to take his oxygen on those trips. He rarely used it just walking around the house.
He did make a serious suicide attempt six years ago (our daughter and granddaughter had died), but after seeing what it did to me and our son, he promised heтАЩd never do it again. It was only when these exacerbation/flare-up events started this year that he indicated life was getting bad.
Perhaps, just perhaps, if he had received both medications in a timely manner, he would be here today, and we would have had many more years together. We met when we were 16 and had been together ever since. He was 78 when he died.
тАФ Cindy Clements Blewett; Kyle, Texas
Navigating GLP-1 Coverage
Sydney LupkinтАЩs thoughtful article about the obstacles in obtaining weight loss drugs was interesting (Healthcare Helpline: тАЬTrouble Getting Weight Loss Drugs Covered by Insurance? HereтАЩs What To Know,тАЭ June 26). It would have been more helpful had it included a discussion of MedicareтАЩs decision to cover these drugs as of July 1, 2026, and how to navigate the rocky shores of obtaining a prescription that wonтАЩt be denied.
тАФ Sharie Hartman; Manteca, California
Beyond the Veil of Pregnancy Centers
I would like to address the article about a pregnancy resource center providing prenatal care in Sandpoint, Idaho (тАЬReligious Anti-Abortion Center Finds Opportunity in Town Without OB-GYNs,тАЭ May 20). It is unfortunate that many still do not understand what pregnancy resource centers do, nor the high-quality care they provide. While there are some тАЬcrisis pregnancy centersтАЭ that provide limited offerings, most centers are aligned with a national organization like the National Institute of Family and Life Advocates, the Heartbeat Pregnancy Center, or Care Net. All these organizations require centers to have a medical director (a licensed healthcare practitioner) and require that the nurses who perform the ultrasounds have appropriate training. While I am not affiliated with 7B Care Clinic, I am concerned that the article may not have accurately reflected what is provided in such clinics. I offer my experiences to bring further clarity.
I work at a life-affirming womenтАЩs clinic. I am a board-certified family physician. I have delivered approximately 1,000 babies in my career. I have been performing ultrasounds for my patients for over a decade, and fought for this ability under the scrutiny of maternal-fetal medicine specialists, spending time alongside their registered diagnostic medical sonographer technicians, and having my scans reviewed by maternal-fetal medicine physicians. I have practiced medicine in three states over three decades.
Second, while I am life-affirming, I am not тАЬanti-abortion.тАЭ I happen to believe that there are better choices, and I know that some women will still choose abortion, even after hearing all their options. I will gladly see those women for follow-up to answer questions and evaluate for complications тАФ something that the abortion clinics in my area apparently will not do. I say this because that is what the women I see tell me. The clinic that performed the procedure or gave them the pills will not see a patient after the abortion for any follow-up. I have always willingly seen patients for any reason, whether I was working at a private clinic or hospital-owned clinic. That is no different now that I work for a life-affirming womenтАЩs clinic.
We provide a variety of services тАФ free of charge. We are also stepping up to provide prenatal care up to 20 weeks because there is a shortage of obstetrical clinicians in our county. We encourage women to see a clinic where they can be followed throughout the entire pregnancy, if possible, and we are in no way marketing ourselves as competition. We are stepping in to fill the large gap that exists.
Just because the clinic in Sandpoint chooses to respect life does not make it a fake clinic. This clinic seeks to bring in physicians to provide prenatal care. They are bringing in OB-GYNs from Washington state, which has no restrictions on abortion. With this information taken into consideration, I ask you to reconsider any concerns about a clinic bringing board-certified OB-GYNs into an area where there is a shortage.
тАФ James Heid, Vancouver, Washington
The Root of All Good
The article Claudia Boyd-Barrett wrote about how immigrant parentsтАЩ arrests are creating a mental health crisis for children was moving and brought awareness to the mental health challenges faced by them (Growing Up Scared: тАЬArrests of Immigrant Parents Create Mental Health Crisis for Children,тАЭ June 18). It was important to note how every story was different but focused on how much children missed and yearned for their parents to come back home. You also wrote about how it affected them by not having a parental figure in the home. That really touched me. Specifically, JacobтАЩs story and when he listed all the things he missed about his mom but especially being close to her.
I am currently a masterтАЩs student in social work working to become a better ally to the Hispanic immigrant community. IтАЩve seen how being afraid and sad over the immigration policies has affected my friends in this community. Losing a close parent and not being able to have that security with them anymore is hard to go through, and trauma affects children as they grow.
In this article, you have recognized the worth of a person, which is a core principle in social work. These children are worthy and have the right to feel taken care of and secure.
I would love to see more mental health services accessible to immigrant communities and their families. This would benefit children as they learn to cope with their feelings and how to make sense of a new world.
тАФ Stacy Xiong, Athens, Georgia
Bagging a Bargain
Author Susan Jaffe mentioned GoodRx in the article тАЬThousands of Medicare Beneficiaries Thought Their Drug Plan Was Free. Then They Lost ItтАЭ (July 7), but she failed to mention a much better discount drug site, Mark CubanтАЩs costplusdrugs.com, where a 90-day supply of 2.5 milligrams of rivaroxaban, a generic for Xarelto, is available for under $50. This could help the thousands of people who lost coverage through unpaid premiums from Wellcare Value Script obtain their medications. The problem of yearly increasing penalties for losing Part D coverage is something that has to be addressed by the Centers for Medicare & Medicaid Services.
Thanks to ║┌┴╧│╘╣╧═Ї News for the relevant coverage.
тАФ Jackie Button; Miami
Fleshing Out the Details
Your report identifying alpha-gal syndrome as a red meat allergy is accurate in that respect but inadequate in its breadth (тАЬWould Hunters Take a Lyme Disease Vaccine? We Asked,тАЭ June 30). Alpha-gal is an allergic reaction to virtually all mammalian products. If you explore that, youтАЩll find an interesting story, as mammalian products are everywhere, including in pharmaceuticals, cosmetics, and other non-meat products. Alpha-gal is growing rapidly, and too many people, including doctors, do not realize that AGS is far worse than just a red meat allergy.
I suggest you help build understanding of the threat by describing the allergy in the future as an allergy to mammalian products. If you do not think your audience will understand that term, perhaps you can explain that it includes pork and anything derived from animals with hooves. As a former and now retired reporter, I encourage you to cover this allergy because its implications are surprising and scary.
тАФ John Varner, Surry, Virginia
A Sales Tax on Doctor Visits and Medicine? In Missouri, Some Worry
A Sales Tax on Doctor Visits and Medicine? In Missouri, Some Worry
ST. LOUIS тАФ Missouri healthcare advocate Leslie Ortbals and her husband want to start a family, but she worries they canтАЩt afford it. The 27-year-old said she takes 10 medications daily to manage multiple chronic illnesses.
Now she worries the cost of those drugs could rise тАФ not because of price increases, but because of a tax system revamp put on the ballot by the stateтАЩs Republican-dominated legislature and backed by the Republican governor.
Prescription drugs and doctor visits are currently exempt from taxes in the state. But in August, Missouri voters will weigh in on a proposed constitutional amendment to give the legislature the power to replace the stateтАЩs income tax with expanded sales taxes, including on goods and services currently exempt.
тАЬPoliticians want Missourians to trust them when they say not to worry about our medications and healthcare being up for grabs,тАЭ Ortbals said at a June press event organized by Progress MO, a progressive advocacy group.
тАЬI have spent enough time in Jefferson City to know better,тАЭ said Ortbals, who works for a Democratic state legislator but was speaking in her personal capacity. тАЬI have watched them speak about protecting life while making lifesaving healthcare less accessible.тАЭ
Taxes on healthcare are unusual in the United States but not unprecedented. Most states over-the-counter drugs. Illinois, MissouriтАЩs neighbor, prescription drugs. Delaware, ▒с▓╣╖╔▓╣╛▒тАШi, New Mexico, and Washington all on services by physicians, dentists, out-of-hospital nursing providers, and medical laboratories.
Critics of the amendment to eliminate income tax in Missouri say itтАЩd be difficult to make up the lost revenue without also imposing taxes on healthcare. Nearly two-thirds of the stateтАЩs general revenue budget comes from income taxes, about $8.7 billion in 2026. Failing to make up that revenue could lead to steep cuts in state services.
Email Sign-Up
Subscribe to ║┌┴╧│╘╣╧═Ї News' free Morning Briefing.
The proposed tax cut comes at an already precarious time for the state budget. Missouri Gov. Mike Kehoe in spending in this yearтАЩs budget over concerns of lagging revenues. The state legislature has passed a since 2022, including . Federal covid aid has propped up the budget in recent years, but the that the surplus is dwindling. And the state is projected to in federal Medicaid funding over 10 years due to cuts from President Donald TrumpтАЩs signature One Big Beautiful Bill Act.
Proponents of the Missouri income tax proposal, such as of the Show-Me Institute, a conservative think tank, say the cut would in the state, both of which have been flat in recent years. He doubts healthcare would be among the things subject to sales tax. But even if it were, he said, it could be done in ways that wouldnтАЩt target lower-income residents. New Jersey, for example, (excluding reconstructive surgeries), which tend to be performed on wealthier people.
In a statement to ║┌┴╧│╘╣╧═Ї News, Kehoe spokesperson Gabby Picard said the governor тАЬwill never support extending sales taxes on agriculture, healthcare, or real estate,тАЭ noting that the legislature would have to decide what to exempt if the ballot measure passes.
Federal law already prohibits states from imposing taxes on many healthcare services covered by government programs such as Medicare, the federal health insurance program for seniors, and Medicaid, the joint state-federal health insurance program for people with low incomes or disabilities, Picard wrote. More than were insured through those two programs in 2024.
But Jay Hardenbrook, advocacy director for AARP Missouri, argued that raising taxes on healthcare, real estate, and agriculture is the for the amendment, considering the legislature doesnтАЩt need special permission to cut income taxes. He cautioned that because the amendment opens the door to new taxes on anything, it could unleash a тАЬweird feeding frenzyтАЭ with special-interest groups lobbying for exemptions.
тАЬLet’s say we do protect prescription drugs from a tax increase; does that mean that the cost of food goes up?тАЭ Hardenbrook said.
And if the Missouri measure passes and the legislature exempts healthcare and real estate from new taxes, Hardenbrook worries about cuts to state-funded services like home and community-based care.
тАЬWhen I talk about taxes going up, and the price of every good and services going up, that’s the best-case scenario,тАЭ Hardenbrook said. тАЬThe worst-case scenario is that the income tax just goes away, and we just don’t have the money to do the things that we need to do.тАЭ
have no income tax, and Washington taxes only capital gains, but of the Institute on Taxation and Economic Policy, a progressive think tank, said the way Missouri is going about its elimination is nearly unprecedented. Only Alaska has repealed a broad-based personal income tax that had previously accounted for a significant portion of the state budget, Davis said.
тАЬThe situation in Alaska was they struck oil, and they had this gusher of economic activity and tax revenue that resulted from that,тАЭ Davis said. тАЬMissouri has not struck oil.тАЭ
A 2012 tax cut in Kansas that reduced income taxes for individuals and eliminated them for some types of businesses created a large budget hole, prompting lawmakers there to the cuts five years later.
Tsapelas of the Show-Me Institute said MissouriтАЩs income tax elimination wouldnтАЩt happen overnight but would instead be more akin to in the state: phased in and tied to revenue targets that would shield the state from massive budget gaps.
тАЬItтАЩs not as doom and gloom as some people are worried about,тАЭ Tsapelas said.
But Ortbals, the healthcare advocate, said too many Missourians are already delaying medical care because of costs.
тАЬI want a Missouri where young people can afford to stay, where families can afford to grow, where chronic illness does not become financial ruin,тАЭ Ortbals said.
Facing Funding Losses, States Call Out Big Businesses With Employees on Medicaid
Facing Funding Losses, States Call Out Big Businesses With Employees on Medicaid
A Walmart store in Martinez, California, in November 2025. (David Paul Morris/Bloomberg via Getty Images)
As the Trump administrationтАЩs January deadline looms for states to enforce new Medicaid work requirements, some state lawmakers are turning the tables by pushing to publicly name the largest companies that have employees enrolled in the government program covering low-income and disabled people.
California lawmakers an expired law that would require the state to identify companies that employ 100 or more people and have employees enrolled in Medi-Cal, the stateтАЩs Medicaid program. Nevada has had a similar law in place since 2017, though a proposal for one in Oregon stalled when its legislative session ended in March.
The California bill author, Democratic state Sen. Lola Smallwood-Cuevas, said she is deeply troubled by what is going to happen when work requirements kick in. According to the state, out of more than on Medi-Cal will be subject to the rule.
тАЬWe think this is a bill thatтАЩs about fairness,тАЭ Smallwood-Cuevas said. тАЬItтАЩs a basic principle that taxpayers deserve transparency about which large employers are shifting their healthcare costs onto the public.тАЭ
Large employers that regularly top NevadaтАЩs list, such as Walmart and Amazon, have said that the state included part-time and seasonal workers in their counts and that their full-time hourly employees to qualify for Medicaid.
Walmart spokesperson Katrina Proffitt said that the company offers affordable medical coverage to most employees, including eligible part-time workers, and that most of its plans include no-cost virtual care options.
тАЬHealthcare affordability and access to quality care remain real barriers for many Americans, and Walmart continues to be committed to being part of the solution,тАЭ Proffitt said.
The push to name and shame companies reflects dueling narratives about the biggest abusers of the joint state-federal Medicaid program, which reached nearly in government spending in 2024. The Trump administration, led by Centers for Medicare & Medicaid Services Administrator Mehmet Oz, has called out blue states for not doing enough to fight insurer fraud and abuse. State Democratic leaders, meanwhile, are pushing back by calling attention to big employers that donтАЩt offer affordable health benefits, which leaves taxpayers subsidizing healthcare costs for the low-wage workforce.
Some states have considered financial penalties. Democratic New Jersey Gov. Mikie Sherrill signed a bill in June that have at least 50 Medicaid-enrolled employees. Companies with 50 to 249 workers on Medicaid per person, and those with at least 500 will pay $725.
Bills that would have penalized companies with workers enrolled in Medicaid failed in this year.
Email Sign-Up
Subscribe to ║┌┴╧│╘╣╧═Ї News' free Morning Briefing.
In Sacramento, California, Democrats want to figure out a way to make large businesses pay for their employeesтАЩ health coverage. State lawmakers struck a deal with Democratic Gov. Gavin Newsom, who is contemplating a presidential bid as he wraps up his final year in the governorтАЩs office, to explore tax options. Any tax hike would be up to the new governor.
States face of dollars under HR 1, the GOP tax-and-spending law known as the One Big Beautiful Bill Act, notably through that requires nondisabled Medicaid enrollees ages 19 to 64 in most states to prove they are working, volunteering, or going to school at least 80 hours a month to keep their coverage.
Yet federal work requirements are projected to increase the number of uninsured people nationwide by more than 5 million by 2034, according to the . Nebraska and Montana have begun enforcing the rule.
One health policy researcher said employer Medicaid reports highlight the lack of affordable healthcare options available to low-wage workers. More than half of adults enrolled in Medicaid who donтАЩt have dependent children already meet the 80-hour-a-month requirement or face challenges that would likely qualify them for an exemption, .
тАЬThereтАЩs a whole set of people who are working тАФ they may not satisfy the work requirement provisions, they may not get the exemption that theyтАЩre qualified for, and they donтАЩt have access to that employer-sponsored insurance either,тАЭ said Edwin Park, a research professor at the Center for Children and Families at Georgetown University.
Employers Push Back
While employer lists havenтАЩt succeeded in bringing down Medicaid costs, supporters say measuring the burden can be the first step and help lawmakers make the case for further action.
In Nevada, Amazon has employed more Medicaid enrollees than any other company since 2020, according to the stateтАЩs report . For state fiscal year 2025, Walmart, the Clark County School District, the state government, and Tesla rounded out the top five.
Employers that the reports are misleading because they have included part-time and seasonal employees. The stateтАЩs includes only full-time employees, plus those who could not be confirmed as either full- or part-time employees.
That came to 4,914 Amazon employees and 3,503 Walmart workers in Nevada on Medicaid in 2025.
There are no penalties for companies on the list.
Amazon said it pays its workers more than double the $7.25-an-hour federal minimum wage and noted that Medicaid eligibility is based on household income and size rather than an individualтАЩs wage. That means two employees who earn the same pay may have different eligibility depending on whether they have children or live with parents.
тАЬPointing fingers at Amazon over Medicaid is a red herring,тАЭ said spokesperson Alisa Carroll. тАЬWhat really needs to happen is a significant and large increase in the federal minimum wage тАФ that would be a big boost for American families.тАЭ
Nevada Medicaid spent nearly $950 million on healthcare for more than 133,000 full-time employees and more than 140,000 of their dependents. While the total amount spent dipped in fiscal year 2025, the average cost per member per year increased by nearly 17%.
Yvanna Cancela, a former Nevada lawmaker who sponsored the legislation on Medicaid work reports, said the annual reports force an important conversation тАЬabout whether or not this is the kind of economy we want and whether or not it is right or just that people who work full-time donтАЩt make enough to have health insurance.тАЭ
A Fraying Safety Net
Health researchers say that uninsured people delay or skip and that their children may end up losing coverage, too.
One analysis found that more than were enrolled in Medicaid and the ChildrenтАЩs Health Insurance Program this April than in January 2025. California is among the states with the among children.
The loss in healthcare coverage among residents will be compounded by the loss of public food assistance benefits, Smallwood-Cuevas said. is pending in the legislature.
She compared Medi-Cal to a trampoline that has become a тАЬvery tattered kind of fishnetтАЭ overwhelmed by people falling into it. President Donald TrumpтАЩs spending-and-tax law pulls and rips at the safety net, she said.
When people lose food assistance and health benefits, they must choose between paying for medicine and paying for rent, Smallwood-Cuevas said.
тАЬWeтАЩre going to see more people in their cars, more people on the street, and a lot more people in the emergency room,тАЭ she said. тАЬThat is dangerous for all of California.тАЭ
Lawmakers Look To Make Abortion Shield Laws Less Dependent on WhoтАЩs Governor
Lawmakers Look To Make Abortion Shield Laws Less Dependent on WhoтАЩs Governor
Mifepristone is one of two drugs used for medication abortions. Many states have shield laws protecting healthcare providers who prescribe abortion medication for patients in other states. (Kayla Bartkowski/The Boston Globe via Getty Images)
0:000:00
Speed
Embed this player
When Gov. Gavin Newsom, using his , refused to extradite a physician accused of prescribing and mailing abortion pills to a Louisiana woman, he said California would тАЬnot everтАЭ allow тАЬextremist politiciansтАЭ to punish its doctors.
Newsom, who is considering a run for president, has long championed reproductive rights, but state lawmakers in the Democratically controlled California legislature know future governors might not have the same political beliefs.
Republican gubernatorial candidate Steve Hilton, a former Fox News host endorsed by President Donald Trump, has vowed to honor these types of extradition requests from other states if heтАЩs elected, Louisiana тАЬis trying to uphold what its people voted for, and California is undermining it.тАЭ His opponent, Democrat Xavier Becerra, has said he would deny the requests.
Legislation advancing in Sacramento is the latest chapter in a tit for tat thatтАЩs been happening between conservative and liberal states since 2022, when the U.S. Supreme Court overturned Roe v. Wade, ending federal legal protections for abortion.
by state Assembly member Rebecca Bauer-Kahan, which is being heard in committee, would take some decisions out of the governorтАЩs hands, requiring governors to deny extradition requests for healthcare providers who prescribe abortion medication or administer gender-affirming care. It would also shield anyone in California who helped patients travel to California or another state to receive legal care. While opponents cast тАЬshield lawsтАЭ as an incursion on other statesтАЩ authority, supporters of the bill view it as insurance тАФ even with Becerra leading Hilton 52% to 31%, according to by the University of California-Berkeley Institute of Government Studies.
Newsom spokesperson Marissa Saldivar said the governor doesnтАЩt comment on pending legislation. Hilton and Becerra didnтАЩt return calls for comment.
тАЬProtecting providers from prosecution should not rely on shifting political winds or a single personтАЩs decision,тАЭ said Alyssa Sherer, a nurse practitioner who spoke in support of the bill at a Senate committee hearing in June. Sherer is also the medical director at Hey Jane, a telehealth medication abortion provider.
Thirteen states have banned abortion outright, and 28 other states ban abortion somewhere between six weeks and viability. At the same time, other states that allow abortion have enacted shield laws to protect doctors and nurses from liability when they prescribe across state lines.
People living in states with total abortion bans are increasingly getting abortion pills prescribed via telehealth, from 74,000 abortions in 2024 to 92,000 abortions in 2025, according to the Guttmacher Institute, citing numbers from its Monthly Abortion Provision Study.
Critics of shield laws say that states have a legitimate interest in enforcing their own statutes and that such laws represent an attempt by some states, like California, to nullify the legal decisions of others.
тАЬIf California says, тАШWeтАЩre not going to honor any other stateтАЩs laws. WeтАЩre going to ship abortion pills into your states. You canтАЩt have a law that says abortion is illegal,тАЩ I donтАЩt know тАФ that doesnтАЩt seem like a workable situation,тАЭ said Greg Burt, who is vice president of the California Family Council and has spoken in opposition to shield laws at the State Capitol.
Email Sign-Up
Subscribe to ║┌┴╧│╘╣╧═Ї News' free Morning Briefing.
Twenty-one other states and Washington, D.C., have similar shield laws, but Arizona, California, Michigan, North Carolina, and PennsylvaniaтАЩs rely on an executive order, which could be reversed by a successor, according to the Guttmacher Institute.
Amanda Barrow, a senior staff attorney at the Center on Reproductive Health, Law, and Policy at UCLA Law, said passing extradition protections would put California on firmer footing, because an executive order тАЬcould be revoked by a governor who is anti-abortion or anti-gender-affirming-care.тАЭ
Hilton has said he would do just that if elected.
тАЬJust as I wouldnтАЩt want to see Louisiana coming in and undermining something that we voted for here in California,тАЭ the GOP candidate told KQED in January.
During a , Becerra said he was strident about protecting reproductive rights as the stateтАЩs attorney general. тАЬAbsolutely no,тАЭ Becerra said of allowing California physicians to be extradited.
This year, ▒с▓╣╖╔▓╣╛▒тАШi to its existing shield laws. And Oregon , including banning law enforcement from cooperating with out-of-state or federal investigations into care thatтАЩs legal in the state.
But Republican legislators in conservative states have cast telehealth visits as an end run around their laws. And some have moved to restrict abortion pill access.
The governors of , , and have signed bills this year that criminalize the sale, purchase, or distribution of medication that induces an abortion. Those states make it a felony to provide medication abortion drugs to people who are seeking to end a pregnancy. The laws impose up to 10 years in prison with potentially tens of thousands of dollars in fines.
Mississippi amended the stateтАЩs controlled substances code to add abortion pills as a criminal category. Although the state already prohibits abortion broadly, the measure specifically addresses distribution, which could subject out-of-state providers to prosecution.
In January, Louisiana a California doctor, Remy Coeytaux, mailing abortion pills to a patient. Newsom denied the request. Likewise, New York Gov. Kathy Hochul denied LouisianaтАЩs February 2025 extradition request for a .
Texas has taken a slightly different legal tact. Attorney General Ken Paxton, a Republican running for the U.S. Senate, obtained a default judgment of more than $100,000 against the New York doctor targeted by Louisiana, but a , citing New YorkтАЩs shield law. Neither Paxton nor Louisiana Attorney General Liz Murrill responded to requests for comment.
Fear of being charged with a crime for providing quality medical care is contributing to physicians leaving medicine, said Sacramento emergency room doctor Kamara Graham, who is vice president of the California chapter of the American College of Emergency Physicians, which is supporting the bill.
тАЬItтАЩs really conflicting and hard for us to weigh that concern of: Will I get extradited and charged and potentially be taken away from my family? Or do I do the right thing for my patient?тАЭ Graham said.
The availability of medication used in most abortions could soon change nationwide. Under the leadership of Health and Human Services Secretary Robert F. Kennedy Jr., the Food and Drug Administration it is conducting a safety review of mifepristone, one of two medications in pill form that is used in most U.S. abortions. The FDA maintains the drug is safe and effective.
If the FDA were to decide that mifepristone is not safe, such a ruling would supersede state laws, even in states where abortion is legal. If mifepristone is restricted, many telehealth groups have said they would switch to using only the other medication, misoprostol.
тАЬThe elephant in the room is whether the Trump administration, particularly after the midterms, makes some kind of move to put national limits on access to abortions,тАЭ said Mary Ziegler, a law professor at UC-Davis who has written several books on reproductive health law.
тАЬNot everything is something that the legislature can solve for,тАЭ Ziegler said, тАЬbecause there’s some uncertainty about how the federal courts are going to react to all of this.тАЭ