But the doctors couldn’t intervene, she said. The fetus still had a heartbeat and it was a Catholic hospital, subject to the “ for Catholic Health Care Services” that prohibit or limit procedures like abortion that the church deems “immoral” or “intrinsically evil,” according to its interpretation of the Bible.
“I remember asking the doctors. And they were like, ‘Well, the baby still has a heartbeat. We can’t do anything,’” said Maldonado, now working as a nurse midwife in California, who asked them: “What do you mean we can’t do anything? This baby’s not going to survive.”
The woman was hospitalized for days before going into labor, Maldonado said, and the baby died.
Ascension declined to comment for this article.
The Catholic Church’s directives are often at odds with accepted medical standards, especially in areas of reproductive health, according to physicians and other medical practitioners.
The American College of Obstetricians and Gynecologists’ for managing pre-labor rupture of membranes, in which a patient’s water breaks before labor begins, state that women should be offered options, including ending the pregnancy.
Maldonado felt her patient made her wishes clear.
“Under the ideal medical practice, that patient should be helped to obtain an appropriate method of terminating the pregnancy,” said Christian Pettker, a professor of obstetrics, gynecology, and reproductive sciences at the Yale School of Medicine, who helped author the guidelines.
He said, “It would be perfectly medically appropriate to do a termination of pregnancy before the cessation of cardiac activity, to avoid the health risks to the pregnant person.”
“Patients are being turned away from necessary care,” said Jennifer Chin, an OB-GYN at UW Medicine in Seattle, because of the “emphasis on these ethical and religious directives.”
They can be a powerful constraint on the care that patients receive at Catholic hospitals, whether emergency treatment when a woman’s health is at risk, or access to birth control and abortions.

More and more women are running into barriers to obtaining care as Catholic health systems have aggressively acquired secular hospitals in much of the country. Four of the 10 largest U.S. hospital chains by number of beds are Catholic, according to federal data from the Agency for Healthcare Research and Quality. There are just over 600 Catholic general hospitals nationally and roughly 100 more managed by Catholic chains that place some religious limits on care, a ∫⁄¡œ≥‘πœÕ¯ News investigation reveals.
Maldonado’s experience in Maryland came just months before the Supreme Court’s ruling in 2022 to overturn Roe v. Wade, a decision that compounded the impact of Catholic health care restrictions. In its wake, roughly a third of states have banned or severely limited access to abortion, creating a one-two punch for women seeking to prevent pregnancy or to end one. Ironically, some states where Catholic hospitals dominate — such as Washington, Oregon, and Colorado — are now considered medical havens for women in nearby states that have banned abortion.
∫⁄¡œ≥‘πœÕ¯ News analyzed state-level birth data to discover that more than half a million babies are born each year in the U.S. in Catholic-run hospitals, including those owned by CommonSpirit Health, Ascension, Trinity Health, and Providence St. Joseph Health. That’s 16% of all hospital births each year, with rates in 10 states exceeding 30%. In Washington, half of all babies are born at such hospitals, the highest share in the country.
“We had many instances where people would have to get in their car to drive to us while they were bleeding, or patients who had had their water bags broken for up to five days or even up to a week,” said Chin, who has treated patients turned away by Catholic hospitals.
Physicians who turned away patients like that “were going against evidence-based care and going against what they had been taught in medical school and residency,” she said, “but felt that they had to provide a certain type of care — or lack of care — just because of the strength of the ethical and religious directives.”
Following religious mandates can be dangerous, Chin and other clinicians said.

When a patient has chosen to end a pregnancy after the amniotic sac — or water — has broken, Pettker said, “any delay that might be added to a procedure that is inevitably going to happen places that person at risk of serious, life-threatening complications,” including sepsis and organ infection.
Reporters analyzed American Hospital Association data as of August and used Catholic Health Association directories, news reports, government documents, and hospital websites and other materials to determine which hospitals are Catholic or part of Catholic systems, and gathered birth data from state health departments and hospital associations. They interviewed patients, medical providers, academic experts, advocacy organizations, and attorneys, and reviewed hundreds of pages of court and government records and health institutions to understand how the directives affect patient care.
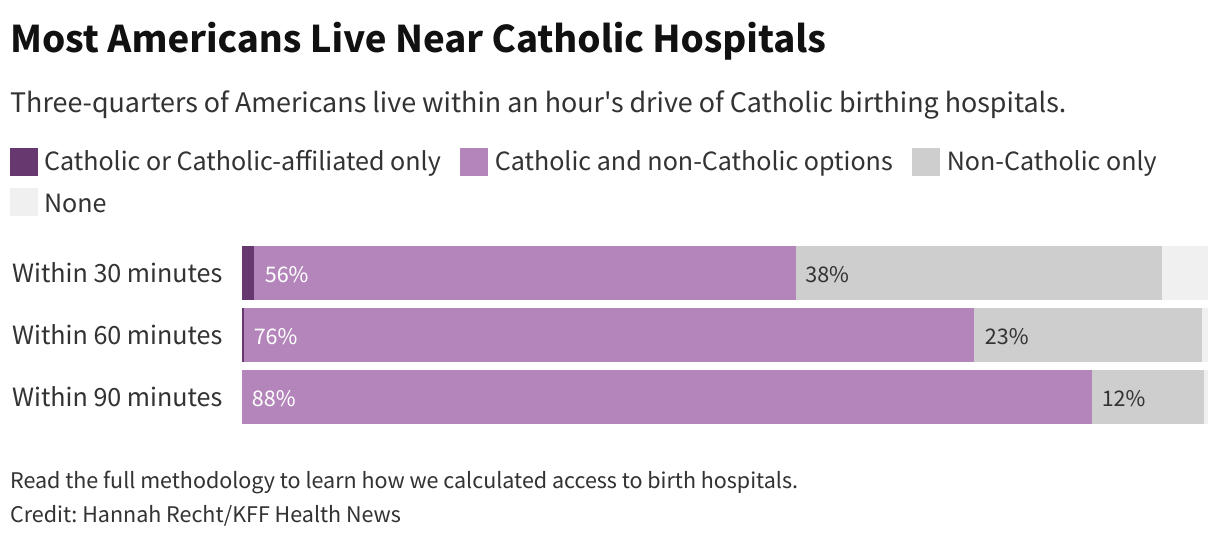
Nationally, nearly 800,000 people have only Catholic or Catholic-affiliated birth hospitals within an hour’s drive, according to ∫⁄¡œ≥‘πœÕ¯ News’ analysis. For example, that’s true of 1 in 10 North Dakotans. In South Dakota, it’s 1 in 20. When care is more than an hour away, academic researchers often define the area as a . Pregnant women who must drive farther to a delivery facility are at higher risk of harm to themselves or their fetus, .
Many Americans don’t have a choice — non-Catholic hospitals are too far to reach in an emergency or aren’t in their insurance networks. Ambulances may take patients to a Catholic facility without giving them a say. Women often don’t know that hospitals are affiliated with the Catholic Church or that they restrict reproductive care, .
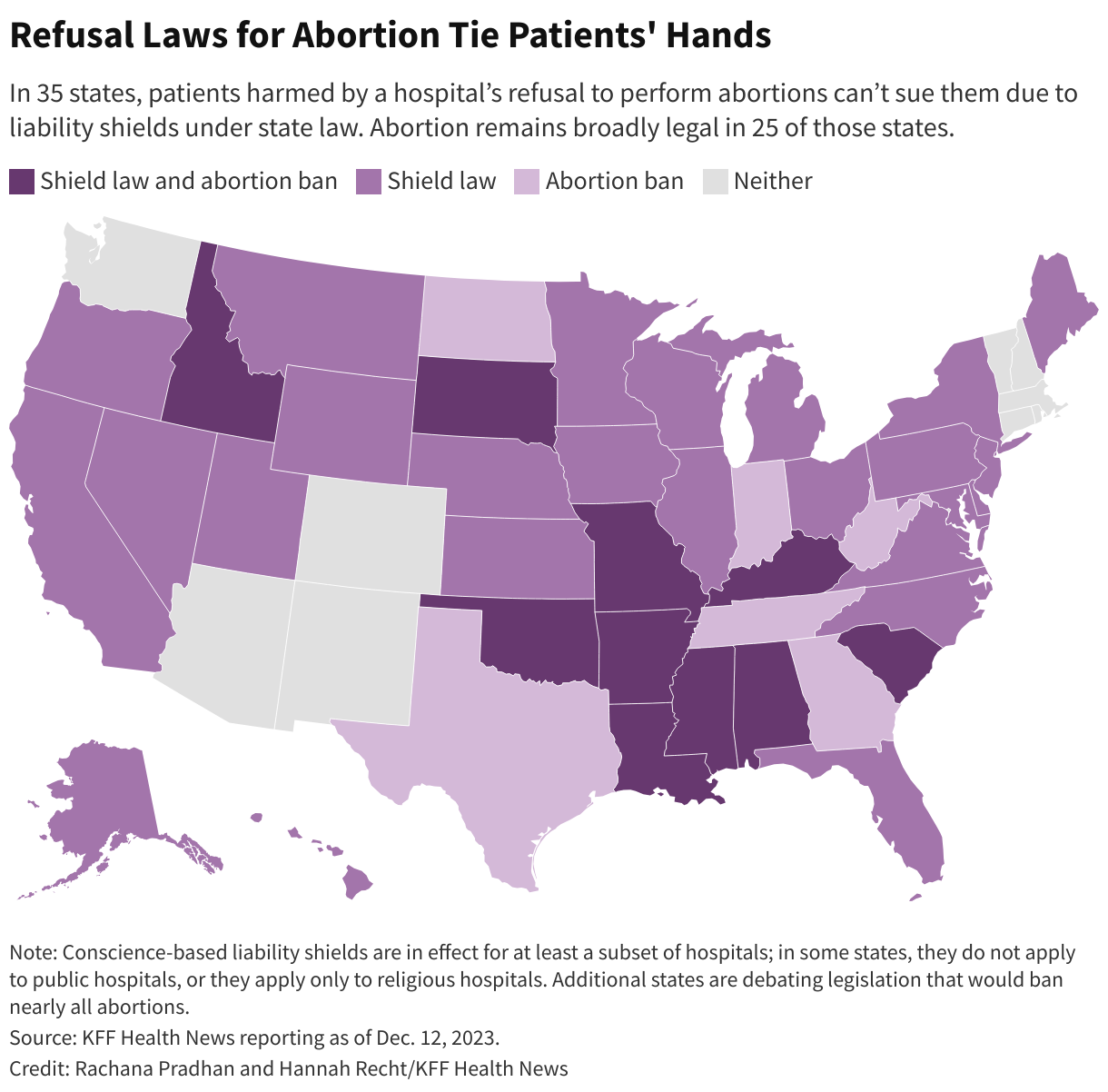
And, in most of the country, state laws shield at least some hospitals from lawsuits for not performing procedures they object to on religious grounds, leaving little recourse for patients who were harmed because care was withheld. Thirty-five states prevent patients from suing hospitals for not providing abortions, including 25 states where abortion remains broadly legal. About half of those laws don’t include exceptions for emergencies, ectopic pregnancies, or miscarriages. Sixteen states prohibit lawsuits against hospitals for refusing to perform sterilization procedures.
“It’s hard for the ordinary citizen to understand, ‘Well, what difference does it make if my hospital is bought by this other big health system, as long as it stays open? That’s all I care about,’” said Erin Fuse Brown, who is the director of the Center for Law, Health & Society at Georgia State University and an expert in health care consolidation. Catholic directives also ban medical aid in dying for terminally ill patients.
People “may not realize that they’re losing access to important services, like reproductive health [and] end-of-life care,” she said.
‘Our Faith-Based Health Care Ministry’
After the Supreme Court ended the constitutional right to abortion in June 2022, Michigan resident Kalaina Sullivan wanted surgery to permanently prevent pregnancy.

Michigan voters in November enshrined the right to abortion under the state constitution, but the state’s concentration of Catholic hospitals means people like Sullivan sometimes still struggle to obtain reproductive health care.
Because her doctor worked for the Catholic chain Trinity Health, the nation’s fourth-largest hospital system, she had the surgery with a different doctor at North Ottawa Community Health System, an independent hospital near the shores of Lake Michigan.
Less than two months later, that, too, became a Catholic hospital, newly acquired by Trinity.
To mark the transition, Cory Mitchell, who at the time was the mission leader of Trinity Health Muskegon, stood before his new colleagues and offered a blessing.
“The work of your hands is what makes our faith-based health care ministry possible,” he said, according to a video of the ceremony Trinity Health provided to ∫⁄¡œ≥‘πœÕ¯ News. “May these hands continue to bring compassion, compassion and healing, to all those they touch.”
Trinity Health declined to answer detailed questions about its merger with North Ottawa Community Health System and the ethical and religious directives. “Our commitment to high-quality, compassionate care means informing our patients of all appropriate care options, and trusting and supporting our physicians to make difficult and medically necessary decisions in the best interest of their patients’ health and safety,” spokesperson Jennifer Amundson said in an emailed statement. “High-quality, safe care is critical for the women in our communities and in cases where a non-critical service is not available at our facility, the physician will transfer care as appropriate.”
Leaders in Catholic-based health systems have hammered home the importance of the church’s directives, which are issued by the U.S. Conference of Catholic Bishops, all men, and were first drafted in 1948. The essential view on abortion is as it was in 1948. The last revision, in 2018, added several directives addressing Catholic health institution acquisitions or mergers with non-Catholic ones, including that “whatever comes under control of the Catholic institution — whether by acquisition, governance, or management — must be operated in full accord with the moral teaching of the Catholic Church.”
“While many of the faithful in the local church may not be aware of these requirements for Catholic health care, the local bishop certainly is,” wrote Sister Doris Gottemoeller, a former board member of the Bon Secours Mercy Health system, in a 2023 . “In fact, the bishop should be briefed on a regular basis about the hospital’s activities and strategies.”
Now, for care at a non-Catholic hospital, Sullivan would need to travel nearly 30 miles.
“I don’t see why there’s any reason for me to have to follow the rules of their religion and have that be a part of what’s going on with my body,” she said.
Risks Come With Religion
Nathaniel Hibner, senior director of ethics at the Catholic Health Association, said the ethical and religious directives allow clinicians to provide medically necessary treatments in emergencies. In a pregnancy crisis when a person’s life is at risk, “I do not believe that the ERDs should restrict the physician in acting in the way that they see medically indicated.”
“Catholic health care is committed to the health of all women and mothers who enter into our facilities,” Hibner said.
The directives permit care to cure “a proportionately serious pathological condition of a pregnant woman” even if it would “result in the death of the unborn child.” Hibner demurred when asked who defines what that means and when such care is provided, saying, “for the most part, the physician and the patients are the ones that are having a conversation and dialogue with what is supposed to be medically appropriate.”
It is common for practitioners at any hospital to consult an ethics board about difficult cases — such as whether a teenager with cancer can decline treatment. At Catholic hospitals, providers must ask a board for permission to perform procedures restricted by the religious directives, clinicians and researchers say. For example, could an abortion be performed if a pregnancy threatened the mother’s life?

How and when an ethics consultation occurs depends on the hospital, Hibner said. “That ethics consultation can be initiated by anyone involved in the direct care of that situation — the patient, the surrogate of that patient, the physician, the nurse, the social worker all have the ability to request a consultation,” he said. When asked whether a consultation with an ethics board can occur without a request, he said “sometimes it could.”
How strictly directives are followed can depend on the hospital and the views of the local bishop.
“If the hospital has made a difficult decision about a critical pregnancy or an end-of-life care situation, the bishop should be the first to know about it,” Gottemoeller wrote.
In an interview, Gottemoeller said that even when pregnancy termination decisions are made on sound ethical grounds, not informing the bishop puts him in a bad position and hurts the church. “If there’s a possibility of it being misunderstood, or misinterpreted, or criticized,” Gottemoeller said, the bishop should understand what happened and why “before the newspapers call him and ask him for an opinion.”
“And if he has to say, ‘Well, I think you made a mistake,’ well, all right,” she said. “But don’t let him be blindsided. I mean, we’re one church and the bishop has pastoral concern over everything in his diocese.”

Katherine Parker Bryden, a nurse midwife in Iowa who works for MercyOne, said she regularly tells pregnant patients that the hospital cannot perform tubal sterilization surgery, to prevent future pregnancies, or refer patients to other hospitals that do. MercyOne is one of the largest health systems in Iowa. Nearly half of general hospitals in the state are Catholic or Catholic-affiliated — the highest share among all states.
The National Catholic Bioethics Center, an ethics authority for Catholic health institutions, that referrals for care that go against church teaching would be “immoral.”
“As providers, you’re put in this kind of moral dilemma,” Parker Bryden said. “Am I serving my patients or am I serving the archbishop and the pope?”
In response to questions, MercyOne spokesperson Eve Lederhouse said in an email that its providers “offer care and services that are consistent with the guidelines of a Catholic health system.”
Maria Rodriguez, an OB-GYN professor at Oregon Health & Science University, said that as a resident in the early 2000s at a Catholic hospital she was able to secure permission — what she calls a “pope note” — to sterilize some patients with conditions such as gestational diabetes.
Annie Iriye, a retired OB-GYN in Washington state, said that more than a decade ago she sought permission to administer medication to hasten labor for a patient experiencing a second-trimester miscarriage at a Catholic hospital. She said she was told no because the fetus had a heartbeat. The patient took 10 hours to deliver — time that would have been cut by half, Iriye said, had she been able to follow her own medical training and expertise. During that time, she said, the patient developed an infection.

Iriye and Chin were part of an effort by reproductive rights groups and medical organizations that pushed for a state law to protect physicians if they act against Catholic hospital restrictions. The bill, , was opposed by the Washington State Hospital Association, whose membership includes multiple large Catholic health systems.
State lawmakers in Oregon in 2021 enacted legislation that if they would reduce access to the types of care constrained by Catholic directives. The hospital lobby has . Washington state lawmakers last year, which the hospital association opposes.
Hibner said Catholic hospitals are committed to instituting systemic changes that improve maternal and child health, including access to primary, prenatal, and postpartum care. “Those are the things that I think rural communities really need support and advocacy for,” he said.
Maldonado, the nurse midwife, still thinks of her patient who was forced to stay pregnant with a baby who could not survive. “To feel like she was going to have to fight to have an abortion of a baby that she wanted?” Maldonado said. “It was just horrible.”
∫⁄¡œ≥‘πœÕ¯ News data editor Holly K. Hacker contributed to this report.
Click to open the methodology Methodology
By Hannah Recht
∫⁄¡œ≥‘πœÕ¯ News identified areas of the country where patients have only Catholic hospital options nearby. The “Ethical and Religious Directives for Catholic Health Care Services” — which are issued by the U.S. Conference of Catholic Bishops, all men — dictate how patients receive reproductive care at Catholic health facilities. In our analysis, we focused on hospitals where babies are born.
We constructed a national database of hospital locations, identified which ones are Catholic or Catholic-affiliated, found how many babies are born at each, and calculated how many people live near those hospitals.
Hospital Universe
We identified hospitals in the 50 states and the District of Columbia using the from August 2023. We removed hospitals that had closed or were listed more than once, added hospitals that were not included, and corrected inaccurate or out-of-date information about ownership, primary service type, and location. We excluded federal hospitals, such as military and Indian Health Service facilities, because they are not open to everyone.
Catholic Affiliation
To identify Catholic hospitals, we used the . We also counted as Catholic a handful of hospitals that are not part of this voluntary membership group but explicitly follow the Ethical and Religious Directives, according to their mission statements, websites, or promotional materials.
We also tracked Catholic-affiliated hospitals: those that are owned or managed by a Catholic health system, such as CommonSpirit Health or Trinity Health, and are influenced by the religious directives but do not necessarily adhere to them in full. To identify Catholic-affiliated hospitals, we consulted health system and hospital websites, government documents, and news reports.
We combined both Catholic and Catholic-affiliated hospitals for analysis, in line with about the influence of Catholic directives on health care.
Births
To determine the share of births that occur at Catholic or Catholic-affiliated hospitals, we gathered the latest annual number of births by hospital from state health departments. Where recent data was not publicly available, we submitted records requests for the most recent complete year available.
The resulting data covered births in 2022 for nine states and D.C., births in 2021 for 23 states, births in 2020 for nine states, and births in 2019 for one state. We used data from the 2021 American Hospital Association survey, the latest available at the time of analysis, for the eight remaining states that did not provide birth data in response to our requests. A small number of hospitals have recently opened or closed labor and delivery units. The vast majority of the rest record about the same number of births each year. This means that the results would not be substantially different if data from 2023 were available.
We used this data to calculate the number of babies born in Catholic and Catholic-affiliated hospitals, as well as non-Catholic hospitals by state and nationally.
We used hospitals’ Catholic status as of August 2023 in this analysis. In 10 cases where the hospital had already closed, we used Catholic status at the time of the closure.
Because our analysis focuses on hospital care, we excluded births that occurred in non-hospital settings, such as homes and stand-alone birth centers, as well as federal hospitals.
Several states suppressed data from hospitals with fewer than 10 births due to privacy restrictions. Because those numbers were so low, this suppression had a negligible effect on state-level totals.
Drive-Time Analysis
We obtained hospitals’ geographic coordinates based on addresses in the AHA dataset using geocoder. For addresses that could not be automatically geocoded with a high degree of certainty, we verified coordinates manually using hospital websites and Google Maps.
We calculated the areas within 30, 60, and 90 minutes of travel time from each birth hospital that was open in August 2023 using tools from HERE. We included only hospitals that had 10 or more births as a proxy for hospitals that have labor and delivery units, or where births regularly occur.
The analysis focused on the areas with hospitals within an hour’s drive. Researchers often define hospital deserts as places where one would have to drive an hour or more for hospital care. (For example: [1] “,” [2] “,” [3] “,” [4] “.”)
We combined the drive-time areas to see which areas of the United States have only Catholic or Catholic-affiliated birth hospitals nearby, both Catholic and non-Catholic, non-Catholic only, or none. We then joined these areas to the 2021 census block group shapefile from and removed water bodies using the to calculate the percentage of each census block group that falls within each hospital access category. We calculated the number of people in each area using the 2021 “American Community Survey” block group population totals. For example, if half of a block group’s land area had access to only Catholic or Catholic-affiliated hospitals, then half of the population was counted in that category.
This <a target="_blank" href="/health-industry/catholic-hospitals-affiliates-ethical-religious-directives-reproductive-care/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1801074&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>More than a million Americans have lost coverage through the program for low-income and disabled Americans in the past several weeks, following the end of pandemic protections on April 1, according to the latest Medicaid renewal data from more than 20 states.
After a three-year pause, most states have now resumed checking and dropping those who no longer qualify or don’t complete required paperwork. About 4 in 5 people dropped so far either never returned the paperwork or omitted required documents, federal and state data show.
Xavier Becerra, secretary of the Department of Health and Human Services, decried those numbers sent to state governors on June 12.
“I am deeply concerned with the number of people unnecessarily losing coverage, especially those who appear to have lost coverage for avoidable reasons that State Medicaid offices have the power to prevent or mitigate,” he wrote.
The Biden administration outlined several optional steps states can take to ensure everyone who still qualifies for the safety-net health insurance program stays covered. For instance, states can pause the cancellations to allow more time to reach people who haven’t responded. Health insurance companies that manage Medicaid plans can help their enrollees fill out the paperwork.
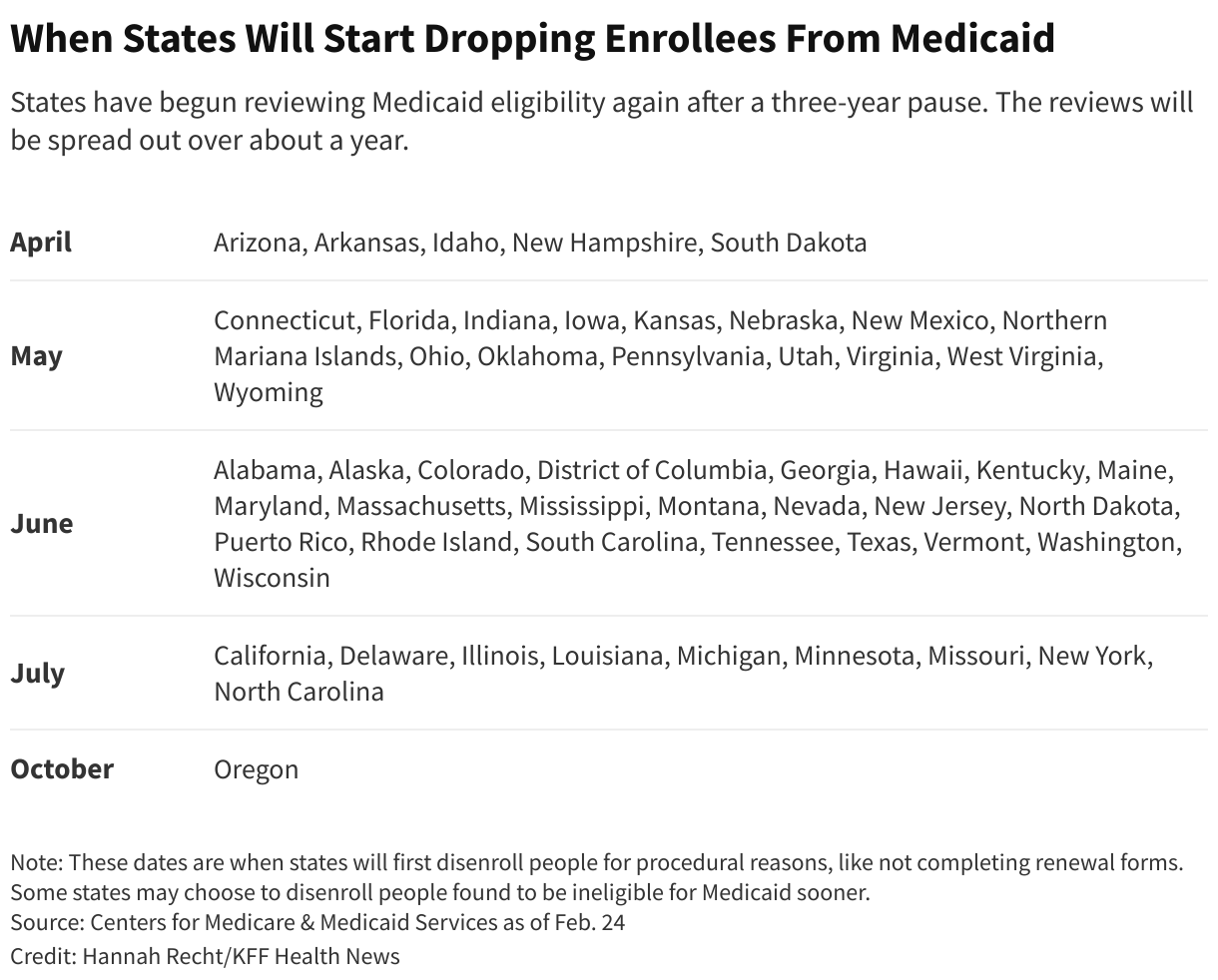
Some states were already choosing to take extra time. Though Wyoming began renewals in May, the state is being “deliberately cautious” and won’t drop people for incomplete paperwork until July or August, state Health Department spokesperson Kim Deti said. Oregon won’t start those cancellations .
Officials in other states have demonstrated no eagerness to slow the cuts.
About 10 percent of Arkansas’ Medicaid and Children’s Health Insurance Program enrollees have already been dropped, nearly all because they didn’t complete paperwork. Arkansas is speeding through the redeterminations in just six months, while most other states are taking about a year, as HHS recommended. Despite outcry from some , Medicaid officials in the state wrote on June 8 that they would people who no longer qualify.
That could be disastrous, said Joan Alker, executive director of Georgetown University’s Center for Children and Families. “My big worry is that we could lose millions of families quickly. It’s going to be very hard to get them back.”
Becerra also wrote that he is “particularly concerned” about children losing coverage, although the administration doesn’t know exactly how many kids have been dropped. States don’t have to report numbers by age to federal authorities, said Dan Tsai, director of the Center for Medicaid and CHIP Services.
Tens of thousands of kids are losing coverage, according to data from states that shared it. In Indiana, of the 53,000 dropped in the first month, a third were kids. In South Dakota, more than half were kids. In Arkansas, nearly 55,000 kids were dropped in the first two months.
Becerra also urged governors to work more directly with families at risk of losing coverage. State agencies should team up with schools, faith-based groups, pharmacies, and other community organizations to help enrollees better understand how to stay on Medicaid, he wrote.
In most states, people who still qualify for Medicaid but lose coverage because of state errors or incomplete paperwork have 90 days to ask for their coverage back.
Some officials view the large number of paperwork-related cancellations as no big deal because people can reapply if they still qualify. But it’s not that simple, Alker said. Many people don’t know their appeal rights, and the grace period doesn’t apply to all adults in several of the hardest-hit states.
Alker said states will temporarily save money from not having to pay for enrollees’ care. But in the meantime, people won’t be able to afford their regular medications. Some will end up in the emergency room sicker than before, she said. “There’s really nothing good that comes out of these gaps in coverage.”
∫⁄¡œ≥‘πœÕ¯ News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF‚Äîan independent source of health policy research, polling, and journalism. Learn more about .This <a target="_blank" href="/health-industry/biden-administration-states-medicaid-cuts-million-dropped/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1703524&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>Under normal circumstances, states review their Medicaid enrollment lists regularly to ensure every recipient qualifies for coverage. But because of a nationwide pause in those reviews during the pandemic, the health insurance program for low-income and disabled Americans kept people covered even if they no longer qualified.
Now, in what’s known as the , states are who stays and who goes. People who are no longer eligible or don’t complete paperwork in time will be dropped.
The overwhelming majority of people who have lost coverage in most states were dropped because of technicalities, not because state officials determined they no longer meet Medicaid income limits. Four out of every five people dropped so far either never returned the paperwork or omitted required documents, according to a ∫⁄¡œ≥‘πœÕ¯ News analysis of data from 11 states that provided details on recent cancellations. Now, lawmakers and advocates are expressing alarm over the volume of people losing coverage and, in some states, calling to pause the process.
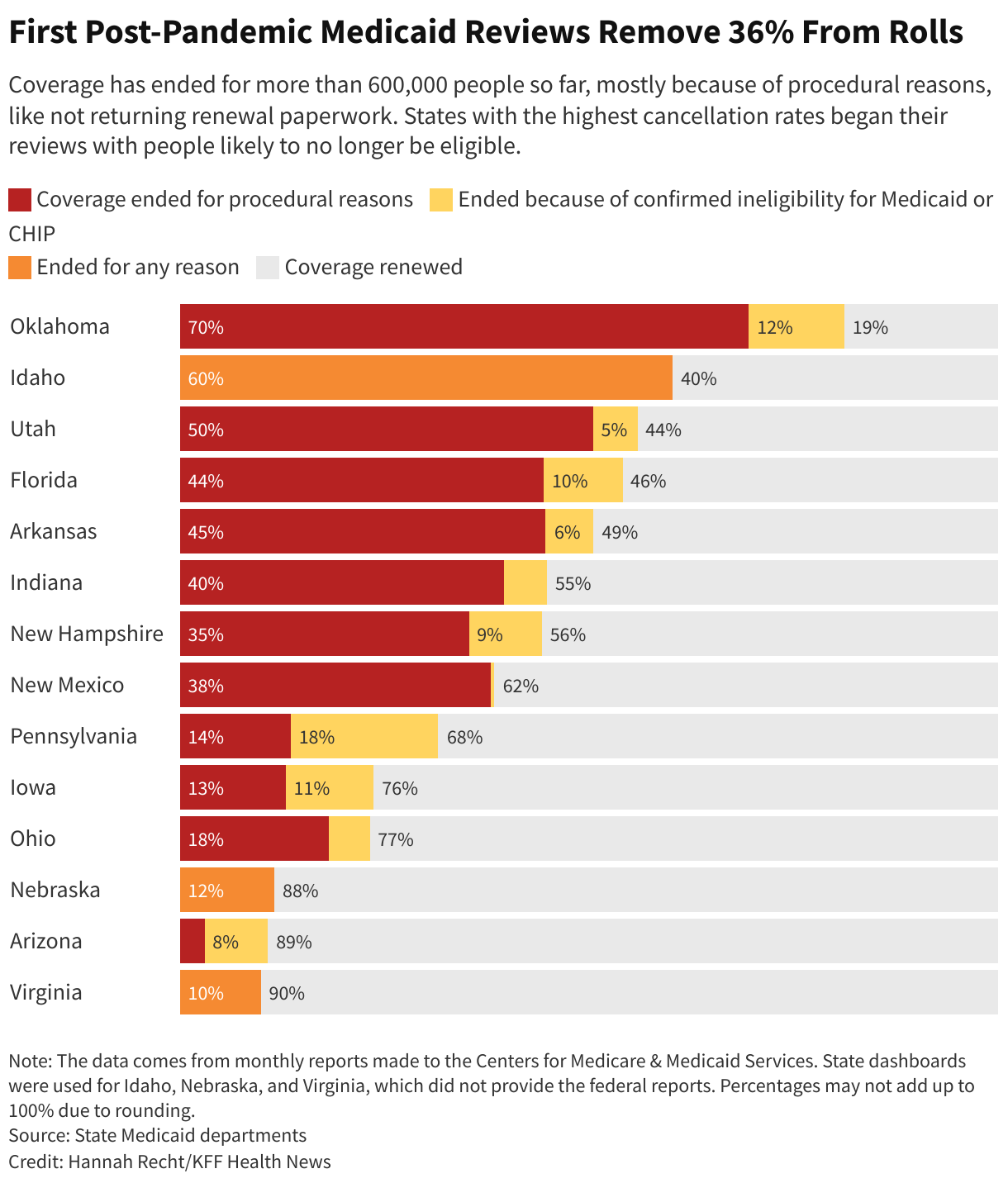
∫⁄¡œ≥‘πœÕ¯ News sought data from the 19 states that started cancellations by May 1. Based on records from 14 states that provided detailed numbers, either in response to a public records request or by posting online, 36% of people whose eligibility was reviewed have been disenrolled.
In Indiana, 53,000 residents lost coverage in the first month of the unwinding, 89% for procedural reasons like not returning renewal forms. State Rep. Ed Clere, a Republican, expressed dismay at those “staggering numbers” in a Medicaid advisory group meeting, repeatedly questioning state officials about forms mailed to out-of-date addresses and urging them to give people more than two weeks’ notice before canceling their coverage.
Clere warned that the cancellations set in motion an avoidable revolving door. Some people dropped from Medicaid will have to forgo filling prescriptions and cancel doctor visits because they can’t afford care. Months down the line, after untreated chronic illnesses spiral out of control, they’ll end up in the emergency room where social workers will need to again help them join the program, he said.
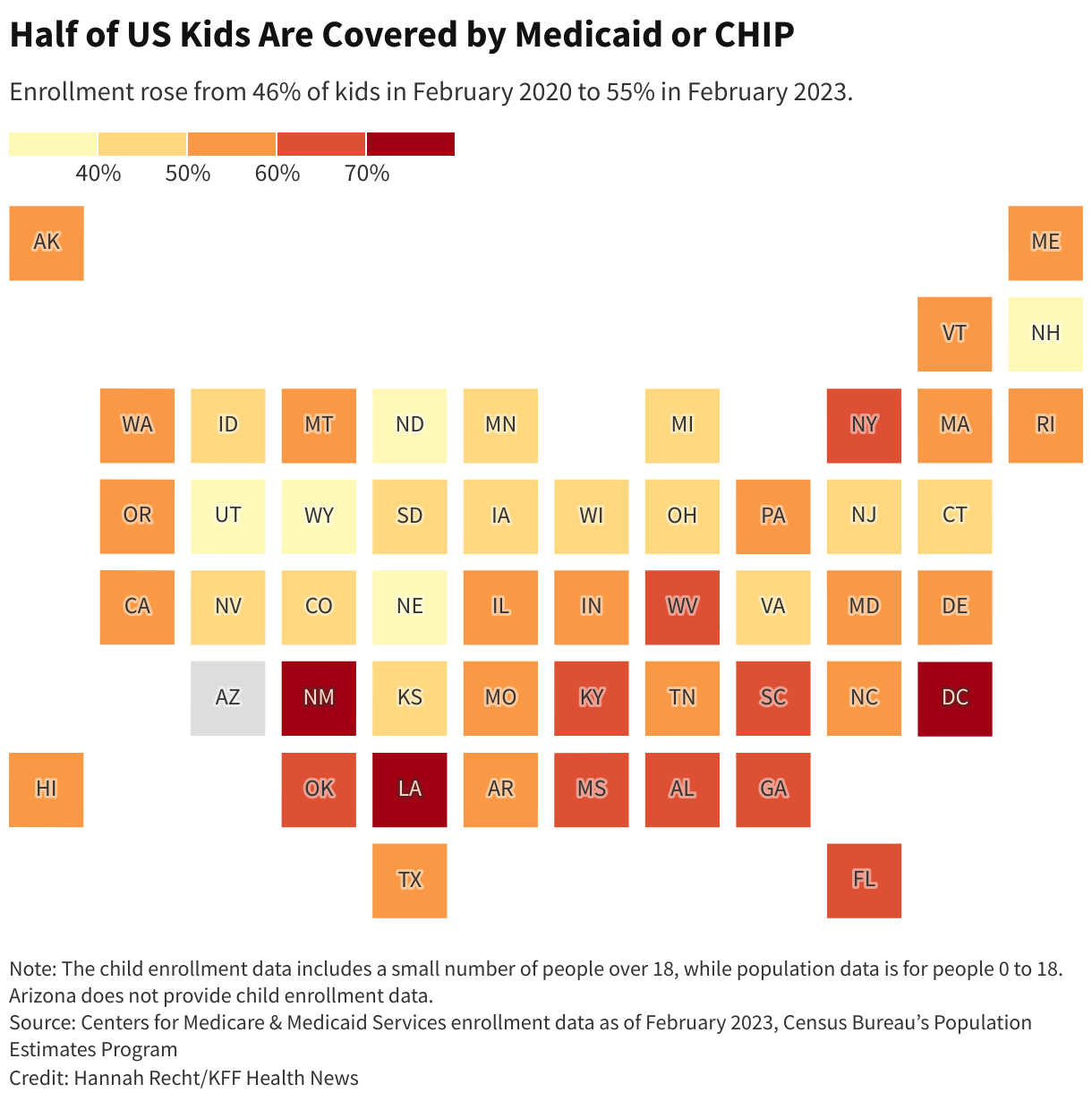
Before the unwinding, more than 1 in 4 Americans — 93 million — were covered by Medicaid or CHIP, the Children’s Health Insurance Program, according to ∫⁄¡œ≥‘πœÕ¯ News’ analysis of the Half of all kids are covered by the programs.
About 15 million people will be dropped over the next year as states review participants’ eligibility in monthly tranches.
Most people through new jobs or qualify for subsidized plans through the Affordable Care Act. But millions of others, including many children, will become uninsured and unable to afford basic prescriptions or preventive care. The uninsured rate among those under 65 is from a historical low of 8.3% today to 9.3% next year, according to the Congressional Budget Office.
Because each state is handling the unwinding differently, the share of enrollees dropped in the first weeks varies widely.
Several states are first reviewing people officials believe are no longer eligible or who haven’t recently used their insurance. High cancellation rates in those states should level out as the agencies move on to people who likely still qualify.
, nearly 56% of people included in early reviews were dropped. In New Hampshire, 44% received cancellation letters within the first two months — almost all for procedural reasons, like not returning paperwork.
But New Hampshire officials found that thousands of people who didn’t fill out the forms indeed earn too much to qualify, according to Henry Lipman, the state’s Medicaid director. They would have been denied anyway. Even so, more people than he expected are not returning renewal forms. “That tells us that we need to change up our strategy,” said Lipman.
In other states, like Virginia and , which aren’t prioritizing renewals by likely eligibility, about 90% have been renewed.
Because of the three-year pause in renewals, many people on Medicaid have never been through the process or they may need to fill out long verification forms, as a recent KFF poll found. Some people moved and didn’t update their contact information.
And while agencies are enrollees who don’t speak English well, many are sending the forms in only a few common languages.
Tens of thousands of children are losing coverage, as , even though some may still qualify for Medicaid or CHIP. In its first month of reviews, South Dakota ended coverage for 10% of all Medicaid and CHIP enrollees in the state. More than half of them were children. In Arkansas, .
Many parents don’t know that limits on household income are significantly higher for children than adults. Parents should fill out renewal forms even if they don’t qualify themselves, said Joan Alker, executive director of the Georgetown University Center for Children and Families.
New Hampshire has moved most families with children to the end of the review process. Lipman, the state’s Medicaid director, said his biggest worry is that a child will end up uninsured. to push kids with serious health conditions and other vulnerable groups to the end of the review line.
But according to Miriam Harmatz, advocacy director and founder of the Florida Health Justice Project, state officials sent cancellation letters to several clients with disabled children who probably still qualify. She’s helping those families appeal.
Nearly 250,000 Floridians reviewed in the first month of the unwinding lost coverage, 82% of them for reasons like incomplete paperwork, the state reported to federal authorities. House Democrats from the state to pause the unwinding.
Advocacy coalitions in both Florida and also have into the review process and a pause on cancellations.
The state is contacting enrollees by phone, email, and text, and continues to process late applications, said Tori Cuddy, a spokesperson for the Florida Department of Children and Families. Cuddy did not respond to questions about issues raised in the petitions.
Federal officials are investigating those complaints and any other problems that emerge, said Dan Tsai, director of the Center for Medicaid & CHIP Services. “If we find that the rules are not being followed, we will take action.”
His agency has to automatically reenroll residents using data from other government programs like unemployment and food assistance when possible. Anyone who can’t be approved through that process must act quickly.
“For the past three years, people have been told to ignore the mail around this, that the renewal was not going to lead to a termination.” Suddenly that mail matters, he said.
Federal law requires states to tell people why they’re losing Medicaid coverage and how to appeal the decision.
Harmatz said some cancellation notices in Florida are vague and could violate due process rules. Letters that she’s seen say “your Medicaid for this period is ending” rather than providing a specific reason for disenrollment, like having too high an income or incomplete paperwork.
If a person requests a hearing before their cancellation takes effect, they can stay covered during the appeals process. Even after being disenrolled, many still have a 90-day window to restore coverage.
In New Hampshire, 13% of people deemed ineligible in the first month have asked for extra time to provide the necessary records. “If you’re eligible for Medicaid, we don’t want you to lose it,” said Lipman.
Clere, the Indiana state representative, pushed his state’s Medicaid officials during the May meeting to immediately make changes to avoid people unnecessarily becoming uninsured. One official responded that they’ll learn and improve over time.
“I’m just concerned that we’re going to be ‘learning’ as a result of people losing coverage,” Clere replied. “So I don’t want to learn at their expense.”
∫⁄¡œ≥‘πœÕ¯ News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF‚Äîan independent source of health policy research, polling, and journalism. Learn more about .This <a target="_blank" href="/insurance/medicaid-unwinding-state-data-coverage-loss/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1697053&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>And that means fewer people will get the potentially lifesaving treatments, experts said.
“I think the numbers will go way down,” said Jill Rosenthal, director of public health policy at the Center for American Progress, a left-leaning think tank. A bill for several hundred dollars or more would lead many people to decide the medication isn’t worth the price, she said.
In response to the unprecedented public health crisis caused by covid, the federal government spent billions of dollars on developing new vaccines and treatments, to swift success: Less than a year after the pandemic was declared, medical workers got their first vaccines. But as many people have refused the shots and stopped wearing masks, the virus still rages and mutates. In 2022 alone, 250,000 Americans from covid, from strokes or diabetes.
But soon the Department of Health and Human Services will stop supplying covid treatments, and pharmacies will purchase and bill for them the same way they do for antibiotic pills or asthma inhalers. Paxlovid is expected to hit the private market in mid-2023, according to HHS plans shared in an October meeting with state health officials and clinicians. Merck’s Lagevrio, a less-effective covid treatment pill, and AstraZeneca’s Evusheld, a preventive therapy for the immunocompromised, are on track to be commercialized sooner, sometime in the winter.
The U.S. government has so far purchased of Paxlovid, priced at about $530 each, a discount for buying in bulk that Pfizer CEO Albert Bourla called “really very attractive” to the federal government in a July earnings call. The drug will cost far more on the private market, although in a statement to KHN, Pfizer declined to share the planned price. The government will also stop paying for the company’s covid vaccine next year — those shots will quadruple in price, from the discount rate the government pays of $30 to about $120.
Bourla told investors in November that he expects the move will make Paxlovid and its covid vaccine “a multibillion-dollars franchise.”
Nearly dying from the virus now are 65 or older. Yet federal law restricts Medicare Part D — the prescription drug program that — from covering the covid treatment pills. The medications are meant for those most at risk of serious illness, including seniors.
Paxlovid and the other treatments are currently available under an emergency use authorization from the FDA, a fast-track review used in extraordinary situations. Although Pfizer in June, the process can take anywhere from several months to years. And Medicare Part D can’t cover any medications without that full stamp of approval.
Paying out-of-pocket would be “a substantial barrier” for seniors on Medicare — the very people who would benefit most from the drug, wrote .
“From a public health perspective, and even from a health care capacity and cost perspective, it would just defy reason to not continue to make these drugs readily available,” said Dr. Larry Madoff, medical director of Massachusetts’ Bureau of Infectious Disease and Laboratory Sciences. He’s hopeful that the federal health agency will find a way to set aside unused doses for seniors and people without insurance.
In mid-November, the White House requested that Congress approve an additional $2.5 billion for covid therapeutics and vaccines to make sure people can afford the medications when they’re no longer free. But there’s little hope it will be approved — the Senate the public health emergency and denied similar requests in recent months.
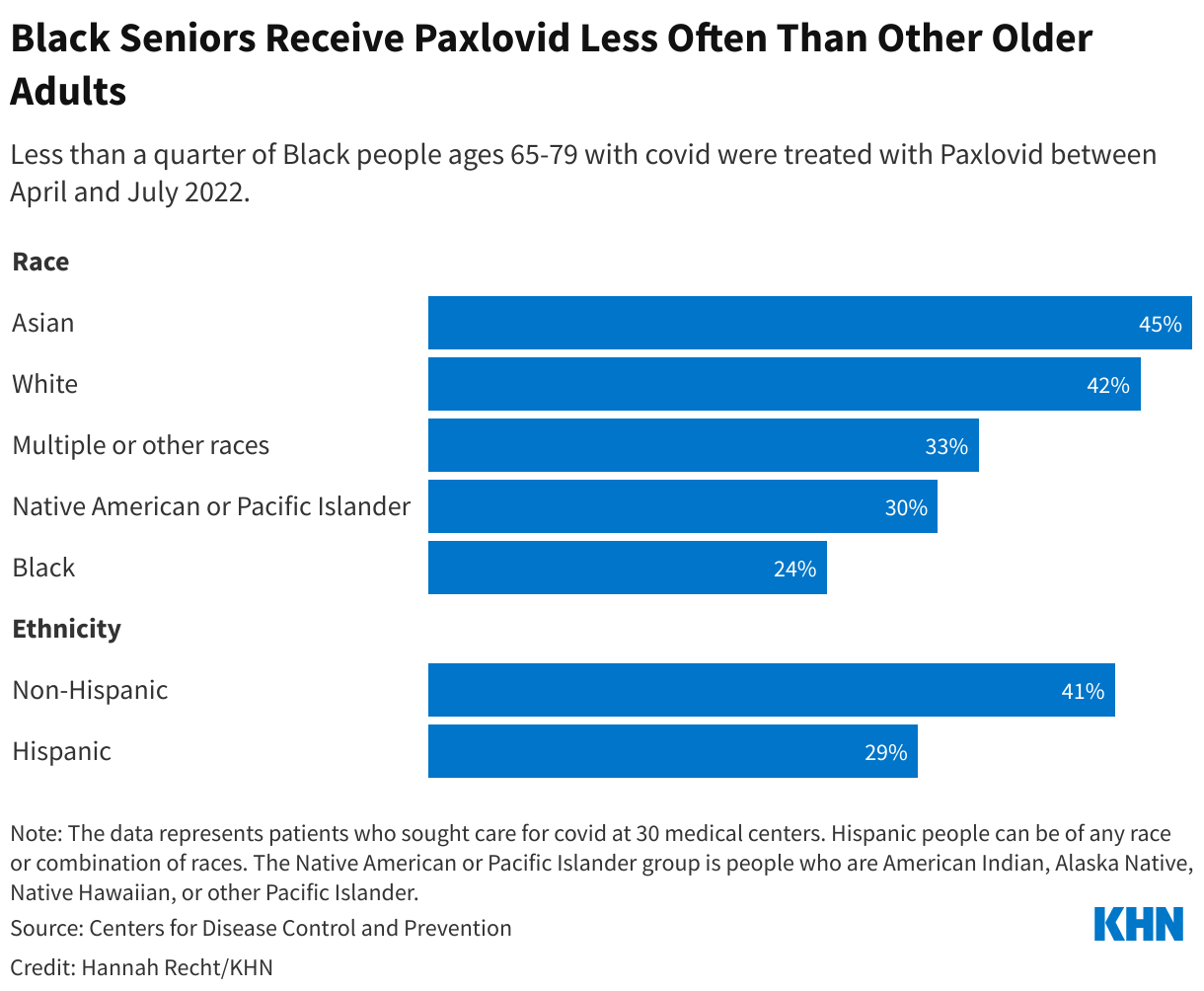
Many Americans have already faced hurdles just getting a prescription for covid treatment. Although the federal government doesn’t track who’s gotten the drug, a using data from 30 medical centers found that Black and Hispanic patients with covid were much less likely to receive Paxlovid than white patients. (Hispanic people can be of any race or combination of races.) And when the government is no longer picking up the tab, experts predict that these gaps by race, income, and geography will widen.
People in Northeastern states used the drug far more often than those in the rest of the country, according to a KHN analysis of Paxlovid use in September and October. But it wasn’t because people in the region were getting sick from covid at much higher rates — instead, many of those states offered better to begin with and created special programs to get Paxlovid to their residents.
About 10 mostly Democratic states and several large counties in the Northeast and elsewhere created free “test-to-treat” programs that allow their residents to get an immediate doctor visit and prescription for treatment after testing positive for covid. In Massachusetts, more than 20,000 residents have used the state’s , which is available seven days a week in 13 languages. Massachusetts, which has the highest insurance rate in the country and relatively low travel times to pharmacies, had the second-highest Paxlovid usage rate among states this fall.
States with higher covid death rates, like Florida and Kentucky, where residents must travel farther for health care and are more likely to be uninsured, used the drug less often. Without no-cost test-to-treat options, residents have struggled to get prescriptions even though the drug itself is still free.

“If you look at access to medications for people who are uninsured, I think that there’s no question that will widen those disparities,” Rosenthal said.
People who get insurance through their jobs could face high copays at the register, too, just as they do for insulin and other expensive or brand-name drugs.
Most private insurance companies will end up covering covid therapeutics to some extent, said Sabrina Corlette, a research professor at Georgetown University’s Center on Health Insurance Reforms. After all, the pills are cheaper than a hospital stay. But for most people who get insurance through their jobs, there are “really no rules at all,” she said. Some insurers could take months to add the drugs to their plans or decide not to pay for them.
And the additional cost means many people will go without the medication. “We know from lots of research that when people face cost sharing for these drugs that they need to take, they will often forgo or cut back,” Corlette said.
One group doesn’t need to worry about sticker shock. Medicaid, the public insurance program for low-income adults and children, will cover the treatments in full until at least early 2024.
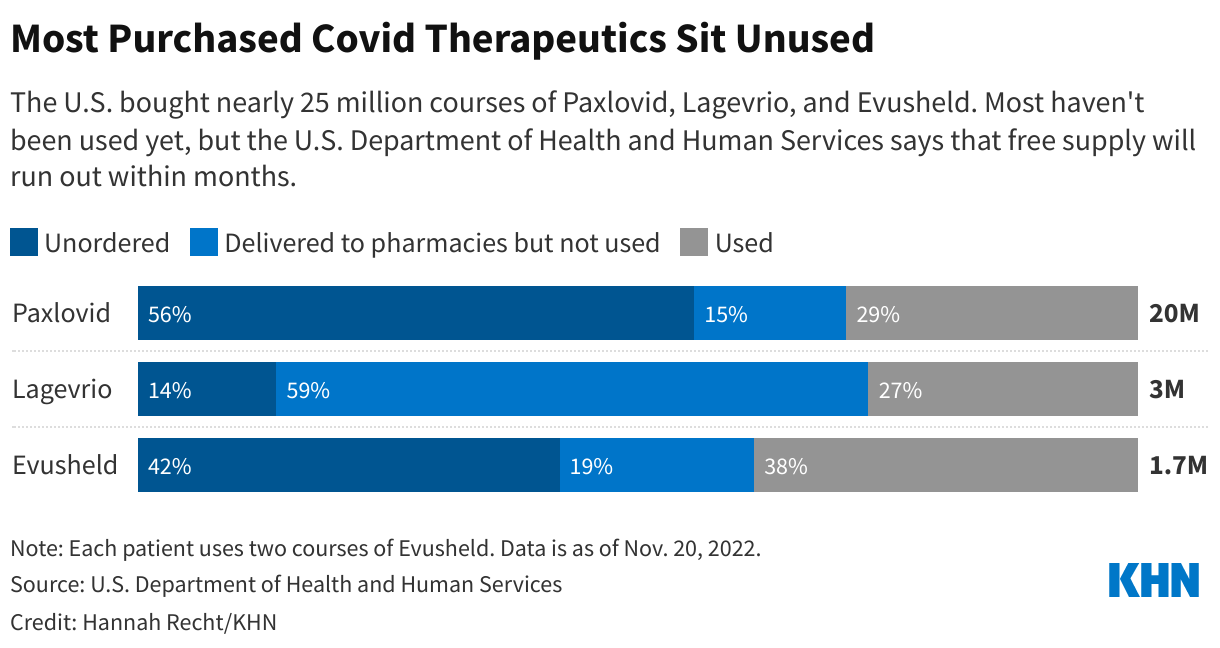
HHS officials could set aside any leftover taxpayer-funded medication for people who can’t afford to pay the full cost, but they haven’t shared any concrete plans to do so. The government purchased 20 million courses of Paxlovid and 3 million of Lagevrio. Fewer than a third have been used, and usage has fallen in recent months, according to KHN’s analysis of the data from HHS.
Sixty percent of the government’s supply of Evusheld is also still available, although the covid prevention therapy is against new strains of the virus. The health department in one state, , has recommended against using it.
HHS did not make officials available for an interview or answer written questions about the commercialization plans.
The government created a potential workaround when they moved bebtelovimab, another covid treatment, to the private market this summer. It now retails for $2,100 per patient. The agency set aside the remaining 60,000 government-purchased doses that hospitals could use to treat uninsured patients in a convoluted . But it’s hard to tell how well that setup would work for Paxlovid: Bebtelovimab was already much less popular, and the FDA on Nov. 30 because it’s less effective against current strains of the virus.
Federal officials and insurance companies would have good reason to make sure patients can continue to afford covid drugs: They’re far cheaper than if patients land in the emergency room.
“The medications are so worthwhile,” said Madoff, the Massachusetts health official. “They’re not expensive in the grand scheme of health care costs.”
∫⁄¡œ≥‘πœÕ¯ News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF‚Äîan independent source of health policy research, polling, and journalism. Learn more about .This <a target="_blank" href="/health-care-costs/paxlovid-covid-sticker-shock-insurance/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1590991&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>Listen to this story:
(.)
A Missouri man who is deaf and blind said a medical bill he didn’t know existed was sent to debt collections, triggering an 11% rise in his home insurance premiums.
An insurer has suspended a blind woman’s coverage every year since 2010 after mailing printed “verification of benefits” forms to her California home that she cannot read, she said. The issues continued even after she got a lawyer involved.
And another insurer kept sending a visually impaired Indiana woman bills she said she could not read, even after her complaint to the Health and Human Services’ Office for Civil Rights led to corrective actions.
Health insurers and health care systems across the U.S. are breaking disability rights laws by sending inaccessible medical bills and notices, a KHN investigation found. The practice hinders the ability of blind Americans to know what they owe, effectively creating a disability tax on their time and finances.
16 and older have a visual disability, according to the National Federation of the Blind. Medical information and bills delivered in an accessible manner is a right protected under various statutes, including the Americans with Disabilities Act, the Affordable Care Act, and the Rehabilitation Act, disability rights legal experts said.
But blind patients told KHN that the letters they receive can be impossible to read if they are not in large print, depending on their level of vision impairment. Some websites have coding incompatible with screen reader technology, which reads text aloud. Some health care systems and insurers fail to mail documents in Braille, which some blind people read by touch.
“I tell them sending me small-print mail is like hiring a mime to communicate to me from outside my window,” Stuart Salvador said over Skype instant messaging. The 37-year-old lives in Greene County, Missouri, and has only residual sight and hearing after a case of shingles when he was 28. “I can tell something is there, but I have no idea what I’m supposed to be getting from that.”
Salvador said it can take up to six hours for him to effectively convert a printed medical bill into Braille. He said he has been sent to collections multiple times by CoxHealth and Mercy hospital systems through their automatic medical debt referral systems after they sent him bills he could not read. As a result, he said, his home insurance carrier raised his annual premium by 11%, costing him an additional $133.51 and hassle.
Nancy Dixon, a spokesperson for Mercy, said that the health system could not find a bill for Salvador that was sent to collections in its records within the past 10 years, and that its policy is to make reasonable accommodations for any patient who requests them. CoxHealth did not respond to requests for comment.
Salvador noted that it’s challenging for him and other visually impaired patients to fight for access to their billing information. If they realize a problem exists, he and other patients told KHN, communicating with the medical systems and insurers can be difficult. But often they may not be aware of the problem until it’s too late. Like Salvador in this instance, some blind patients don’t keep track of written documentation they cannot see, which otherwise might help with a possible legal challenge when overdue billing issues escalate.
Disability rights attorney Albert Elia, who is blind, said blind people stuck with inaccessible bills often are left with two options: to hope for government action or pursue long, costly lawsuits. The National Federation of the Blind and the American Council of the Blind and regarding inaccessible medical information.
Meredith Weaver, a senior staff attorney for Disability Rights Advocates, who helped monitor the implementation of a blind accessibility with health care giant Kaiser Permanente, said her clients often ask for documents to be sent in Braille or be readable by online screen readers. They then typically receive one document that works for them before the cycle begins anew.
“It felt like whack-a-mole to continually make those requests,” she said.
After the terms of the settlement agreement with Kaiser Permanente expired in 2018, Weaver said, she began to hear from clients who faced the same barriers yet again.
Kaiser Permanente spokesperson Marc Brown said that the health system conducted an accessibility review after KHN informed it of Weaver’s comments, and he said the company found “no significant defects in the platform, nor do we know of any inaccessibility issues” that would limit someone from paying their bill or using its website. (KHN is not affiliated with Kaiser Permanente.)
KHN found multiple accessibility issues on the public-facing webpages of Aetna, Anthem Blue Cross, and UnitedHealthcare, major insurers that visually impaired and blind customers flagged as having accessibility problems. The errors, which KHN identified with the help of a tool , a nonprofit web-accessibility organization, include webpage coding that would make it difficult for a blind customer using screen reader technology to shop for a health plan or find an in-network doctor.
After he learned of KHN’s findings, Andrés J. Gallegos, chairman of the , an independent federal agency that advises the White House and Congress, said the council should look more deeply into the issue.
“It’s shocking to the conscience,” he said, noting the law clearly provides for such accessibility protections.
All three insurance companies said they work hard to make their services accessible and strive to fix member issues.
“It’s the year 2022. Everything is being done electronically; everything is being done online,” said Patrick Molloy, a blind 29-year-old in Bucks County, Pennsylvania. “It shouldn’t in theory be terribly difficult to make websites and billing platforms accessible to customers with visual impairments. But it’s the world we live in.”
Getting a lawyer involved doesn’t always solve the problem, said , a web-accessibility specialist at the University of California-Berkeley. The blind 54-year-old sought legal help in early 2020 to stop Anthem Blue Cross from mailing her printed notices she cannot read ‚Äî which sometimes resulted in lapsed benefits because she could not read the request to sign and return them. She now receives some but not all communication through email, which she had requested, and the company’s online portal.
Greco employs an aide to read her mail to help fill in the gaps every other month, but she has still missed insurance notices and bills. She recently raised the aide’s wages to $30 an hour, as Greco wants to ensure she can retain a trustworthy person with all her personal information. But not everyone can afford to hire an aide.
“It makes you feel helpless and it makes you feel dependent on people you might not want to feel dependent on,” she said.

And even when federal entities step in to fix such issues, they persist. Kate Kelly, a 61-year-old in Greenwood, Indiana, who is visually impaired and has hearing loss stemming from multiple sclerosis, was so fed up with receiving multiple bills in standard-sized text from her insurer, Aetna, that she filed a complaint with the HHS Office for Civil Rights in early 2020.
But after the office came to an agreement with Aetna to stop sending her bills in standard-sized text that fall, she said, Aetna soon resumed sending some documents in text too small for her to read. Kelly pushed HHS to reopen her case. This July, records show, the office closed it due to what it said was a lack of jurisdiction, despite its involvement in obtaining the previous resolution.
She said her large-print bills still get delayed ‚Äî one from March just came in August ‚Äî and she is now required to sign for them when they’re delivered. When she tried to use the online portal, she said, her screen reader could not read certain numbers and other information.
“It’s hard to fight back; it’s hard to participate in the system,” she said. “You see why insurance companies get away with it, as it’s not easy to enforce these laws.”
Alex Kepnes, an Aetna spokesperson, said company staffers had reached out to Kelly after KHN’s questions and they “regret the inconvenience that this has caused her.” Kelly said she missed Aetna’s call, and although she called the next day and tried once more, she had yet to hear back as of Nov. 28. She did receive a complaint form from the company ‚Äî in small print she cannot read.
Meanwhile, Kelly said, her utility company manages to get her a bill in large type every month. And she promptly pays it.
∫⁄¡œ≥‘πœÕ¯ News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF‚Äîan independent source of health policy research, polling, and journalism. Learn more about .This <a target="_blank" href="/health-care-costs/disability-tax-medical-bills-inaccessible-blind-americans/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
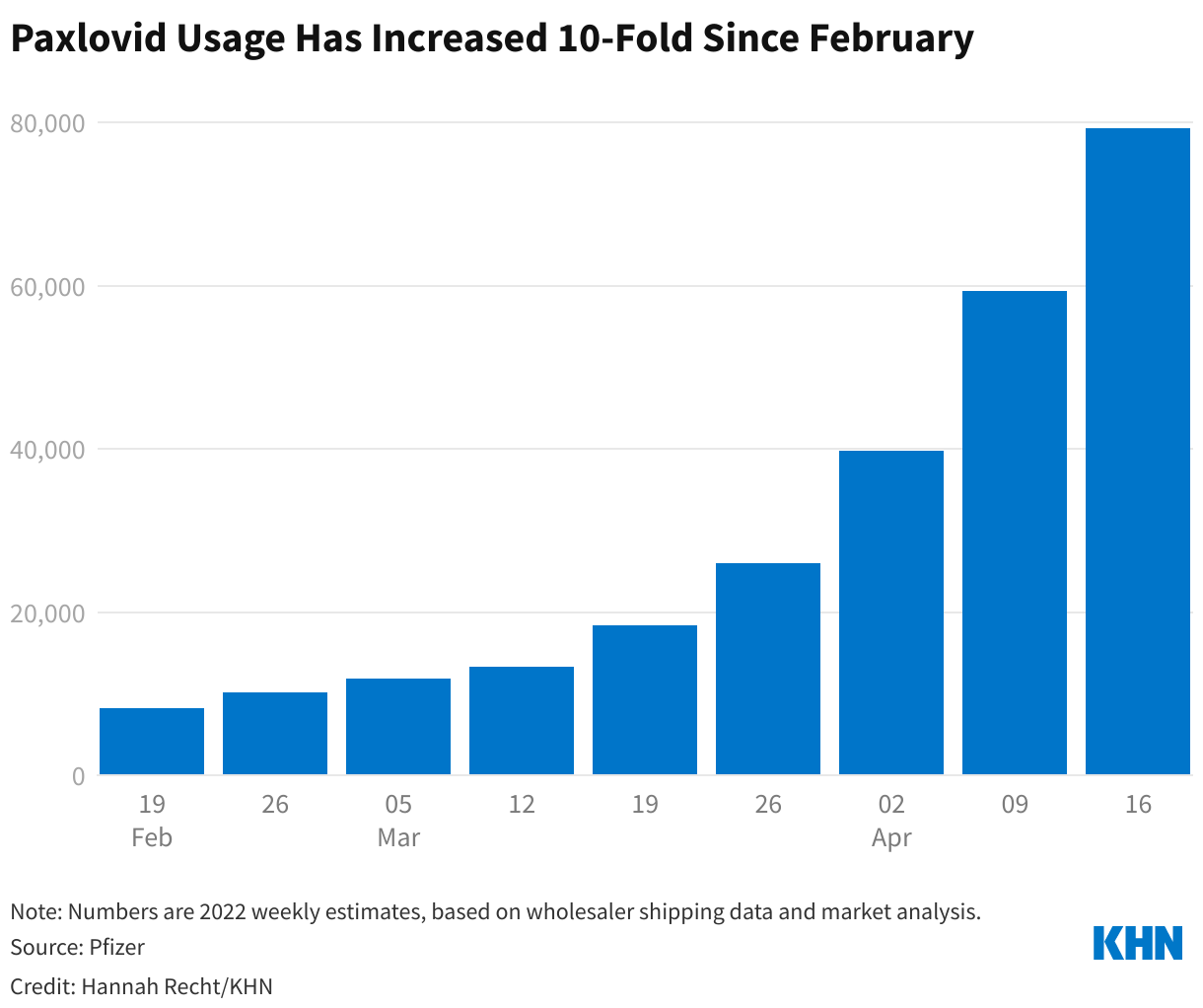
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1586975&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>Pfizer’s Paxlovid pill, along with Merck’s molnupiravir, are aimed at preventing vulnerable patients with mild or moderate covid from becoming sicker or dying. More than 300 Americans still every day.
National supply counts, which the Biden administration has shared sporadically, aren’t the only data local health officials need to ensure their residents can access the treatments. Recent federal changes designed to let large pharmacy chains like CVS and Walgreens efficiently manage their supplies have had an unintended consequence: Now many public health workers are unable to see how many doses have been shipped to their communities or used. And they can’t tell whether the most vulnerable residents are filling prescriptions as often as their wealthier neighbors.
KHN has repeatedly asked Health and Human Services officials to share more detailed covid therapeutic data and to explain how it calculates utilization rates, but they have not shared even the total number of people who have gotten Paxlovid.
So far, the most detailed accounting has come from the drugmakers themselves. Pfizer CEO Albert Bourla reported on a that an estimated 79,000 people received Paxlovid during the week that ended April 22, up from 8,000 a week two months earlier.
 ∫⁄¡œ≥‘πœÕ¯ News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF‚Äîan independent source of health policy research, polling, and journalism. Learn more about .
∫⁄¡œ≥‘πœÕ¯ News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF‚Äîan independent source of health policy research, polling, and journalism. Learn more about .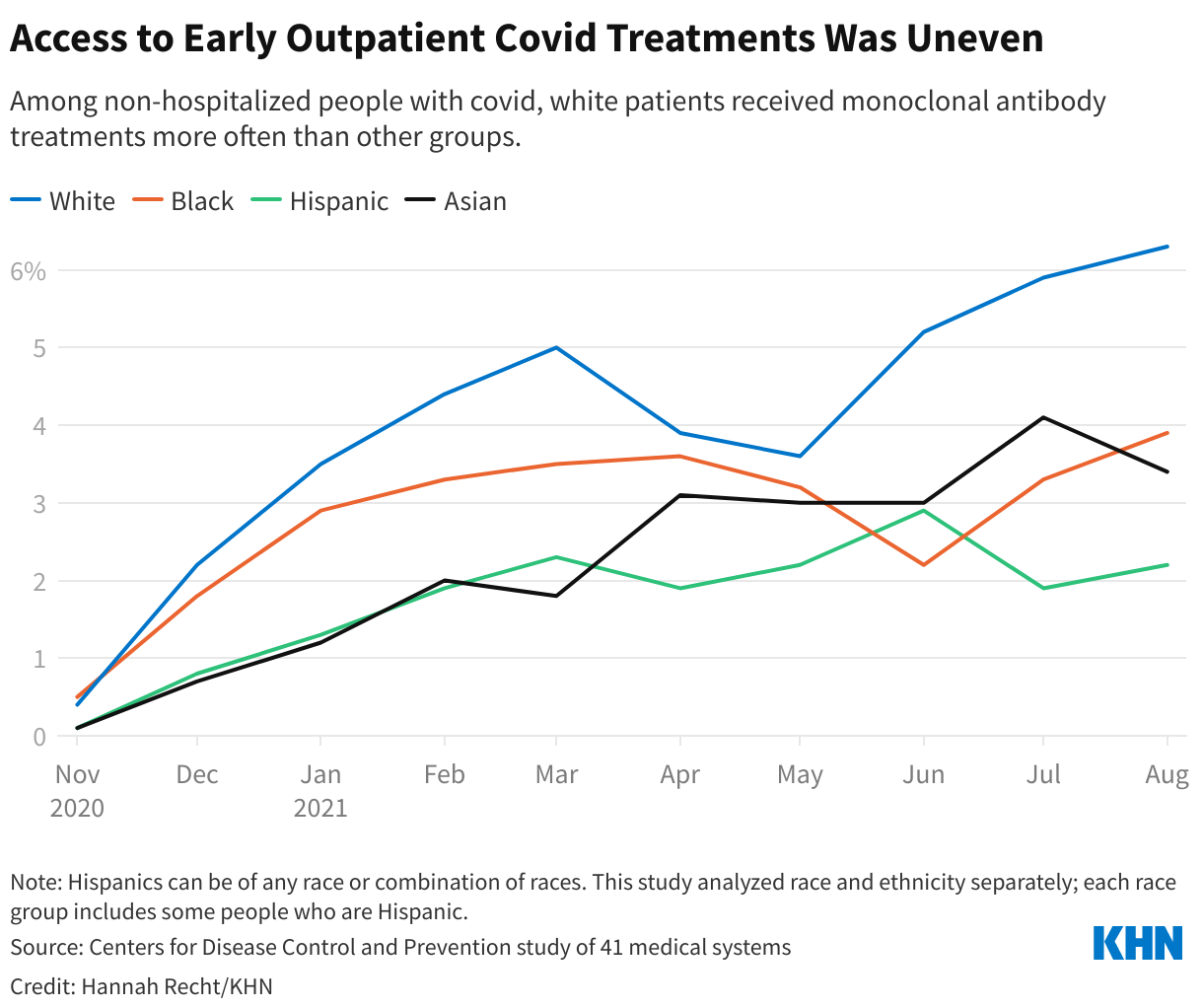
This <a target="_blank" href="/public-health/paxlovid-covid-pill-antiviral-access-data/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1493505&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>Pfizer’s and Merck’s are both designed to be started within five days of someone’s first symptoms. They’re for people who are at high risk of developing severe illness but are not currently hospitalized because of covid-19. Millions of chronically ill, disabled, and older Americans are eligible for the treatments, and Dr. Anthony Fauci of the National Institutes of Health that more people may qualify soon.
The program allows people with covid symptoms to get tested, be prescribed antiviral pills, and fill the prescription all in one visit. The and many state and local health departments direct residents to an online where people can find test-to-treat sites and other pharmacies where they can fill prescriptions.
But large swaths of the country had no test-to-treat pharmacies or health centers listed as of April 14. And the website of the largest participant, CVS, has significant technical issues that make booking an appointment difficult.
Even people who regularly see a doctor may be unable to get a prescription in time, and that’s where the program comes in. Before the pandemic, 28% of Americans a regular source of medical care, with rates even higher for Black and Hispanic Americans.
“All of our public health response relies on lowering the barrier to getting treatments to the right people,” said Dr. Kirsten Bibbins-Domingo, chair of the Department of Epidemiology and Biostatistics at the University of California-San Francisco.
She said the fragmented federal, state, and local public health systems, the U.S. Department of Health and Human Services’ reliance on partners that charge high prices for appointments, and the lack of clear information are stymieing the effort. “The best tools that we have are not going to reach the people who most need them,” she said.
Bibbins-Domingo is also a practicing physician at Zuckerberg San Francisco General Hospital, which she says is not only testing patients for covid and prescribing them antivirals, but also delivering them medications — all the elements of test-to-treat. But the hospital, which largely treats low-income and uninsured patients, doesn’t appear on the federal map. It shows just three locations in San Francisco: two community health centers and one CVS.
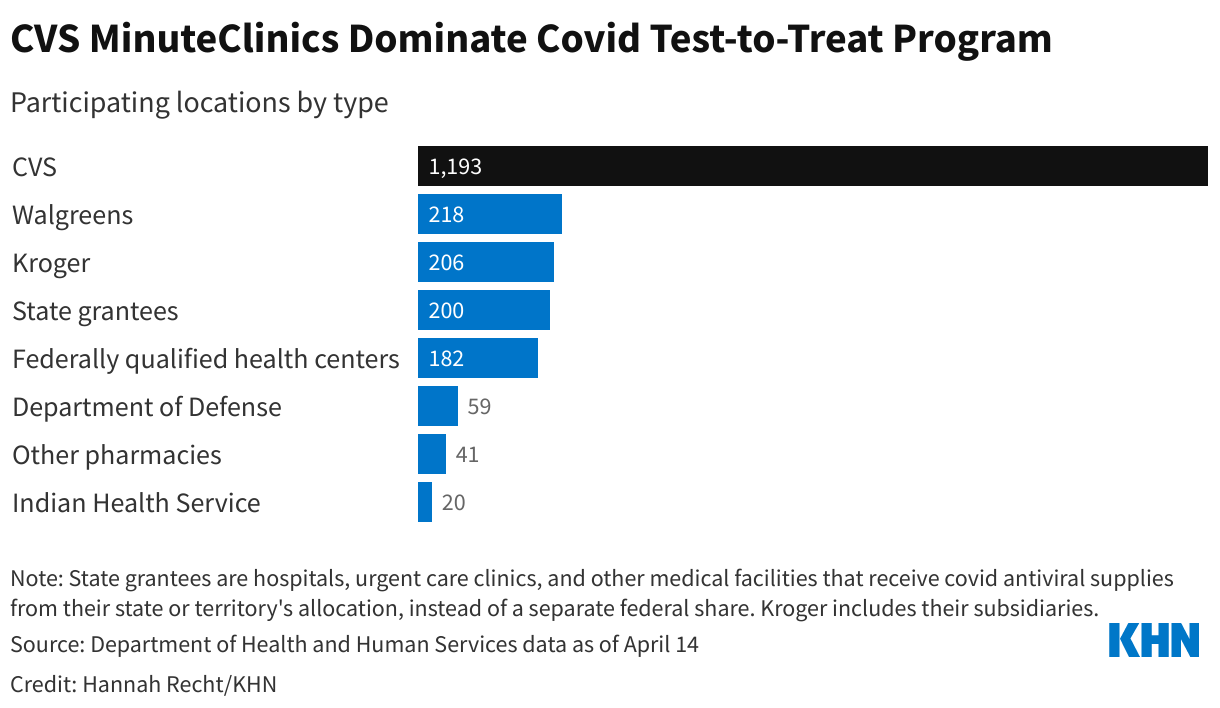
Ninety-one percent of the sites listed on the national map are federal partners: pharmacy chains like CVS, federally qualified health centers, and military and Indian Health Service clinics. HHS has asked state and local health departments to identify , like San Francisco General Hospital, so they can be added. Most states have none of those partners listed yet.
Nationally, CVS MinuteClinics make up more than half of all test-to-treat locations, according to the federal data. The roughly 1,200 clinics, in 35 states and Washington, D.C., are housed under the same roof as CVS pharmacies, where patients can pick up prescriptions for covid antivirals. Walgreens drugstores and Kroger grocery store affiliates run about 400 more sites.
 ∫⁄¡œ≥‘πœÕ¯ News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF‚Äîan independent source of health policy research, polling, and journalism. Learn more about .
∫⁄¡œ≥‘πœÕ¯ News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF‚Äîan independent source of health policy research, polling, and journalism. Learn more about .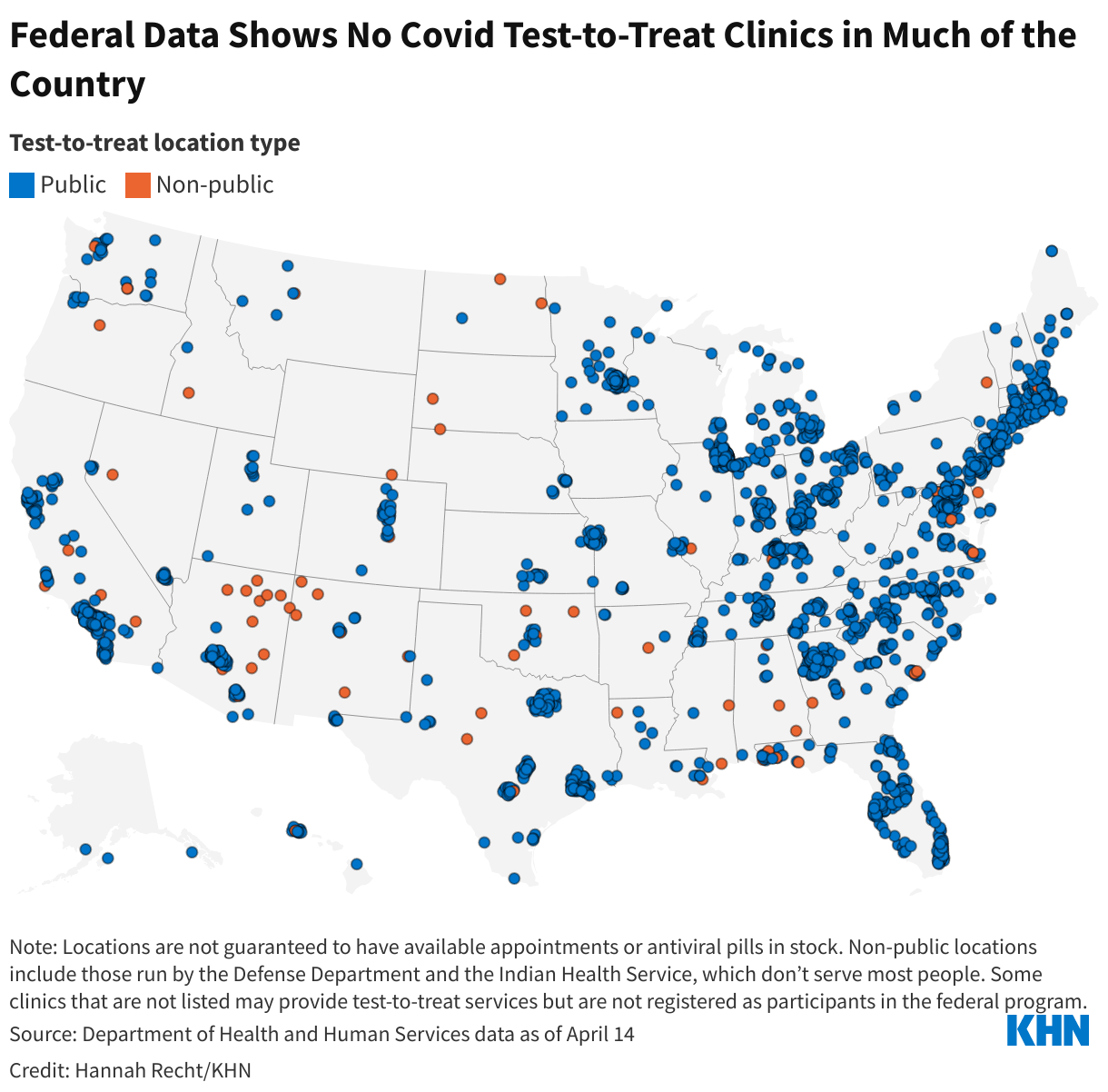
This <a target="_blank" href="/public-health/test-to-treat-biden-covid-failing-patients-pharmacies-cvs/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1479648&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>White House officials had announced March 15 that a planned purchase of more doses would have to be scaled back without new federal funding.
And federal and state health departments aren’t making it easy to find, leaving patients whose hospitals say they don’t have enough of the drug to write desperate tweets and Facebook posts seeking the shots while unused vials sit in the refrigerators of other providers. Few states list on their websites where residents can find Evusheld — most provide no information or link to an incomplete federal map.
The therapy is a pair of monoclonal antibody injections designed to prevent covid infection. It received in December for people 12 and older who are moderately to severely immunocompromised or unable to be vaccinated for medical reasons, more than people. For people who haven’t responded to a covid vaccine, it could offer lifesaving protection.
According to White House officials, by the end of the year.
The week before the White House’s announcement, the Department of Health and Human Services repeatedly told KHN that the problem was supply, not money. HHS spokesperson Elleen Kane stated multiple times that the federal government had bought every dose of Evusheld that AstraZeneca could supply in 2022. But an AstraZeneca spokesperson who declined to be named told KHN that more was available to buy. HHS did not respond to questions about the planned purchase.
HHS expects to receive enough Evusheld for 850,000 people by year’s end, Kane said last week. Even if all those doses come through, the supply would be nowhere near what is needed to treat the millions of people it could benefit.
So far, enough doses to treat 229,000 people have been sent to providers and about one-quarter of that has been used, according to Kane.
After two years of immunocompromised people being left behind by the federal government, “the very least that the Biden administration could do is procure more than enough Evusheld so that everyone who” is eligible can receive the therapy, said , a senior fellow working on health care and disability issues at Data for Progress, a left-leaning think tank.
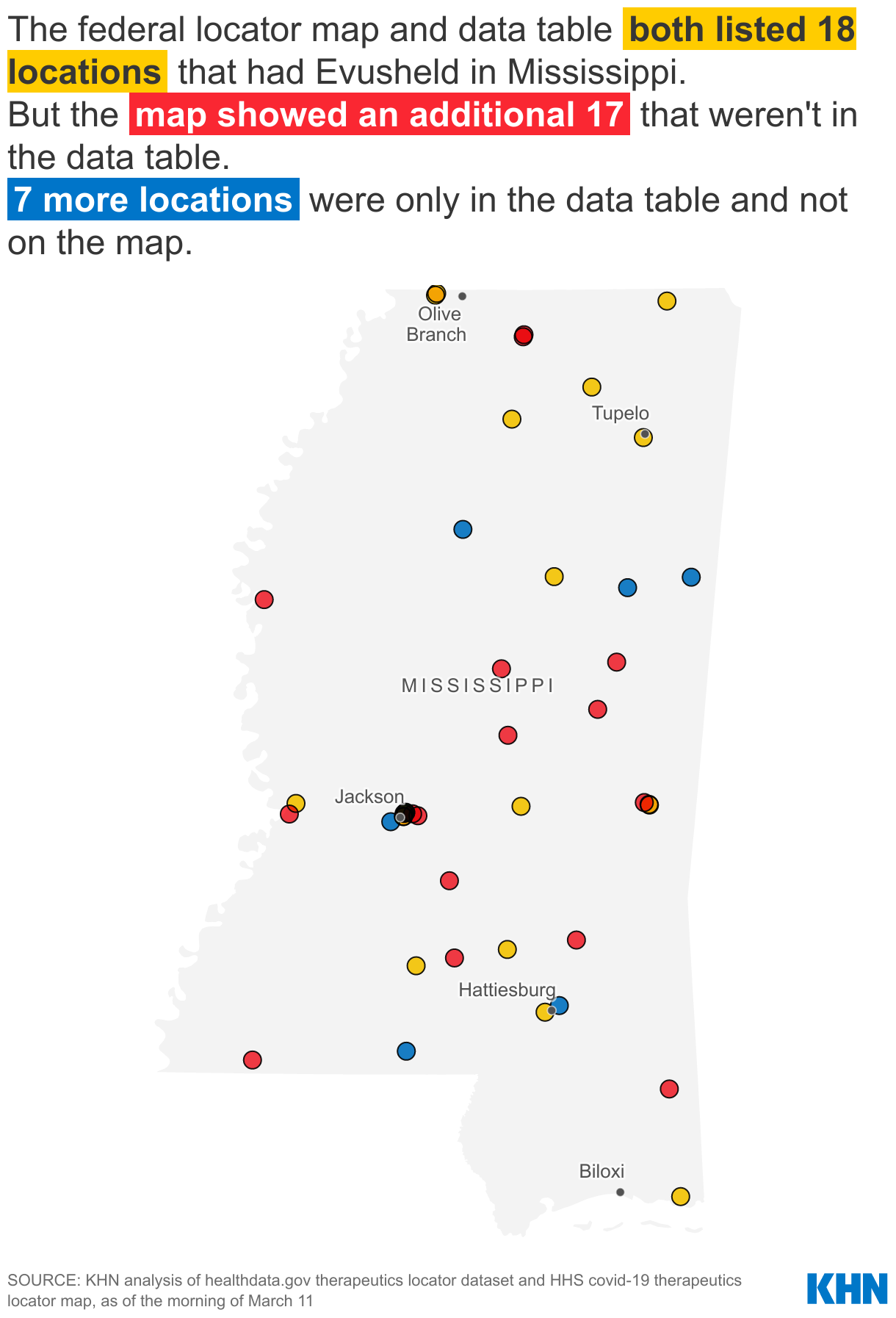
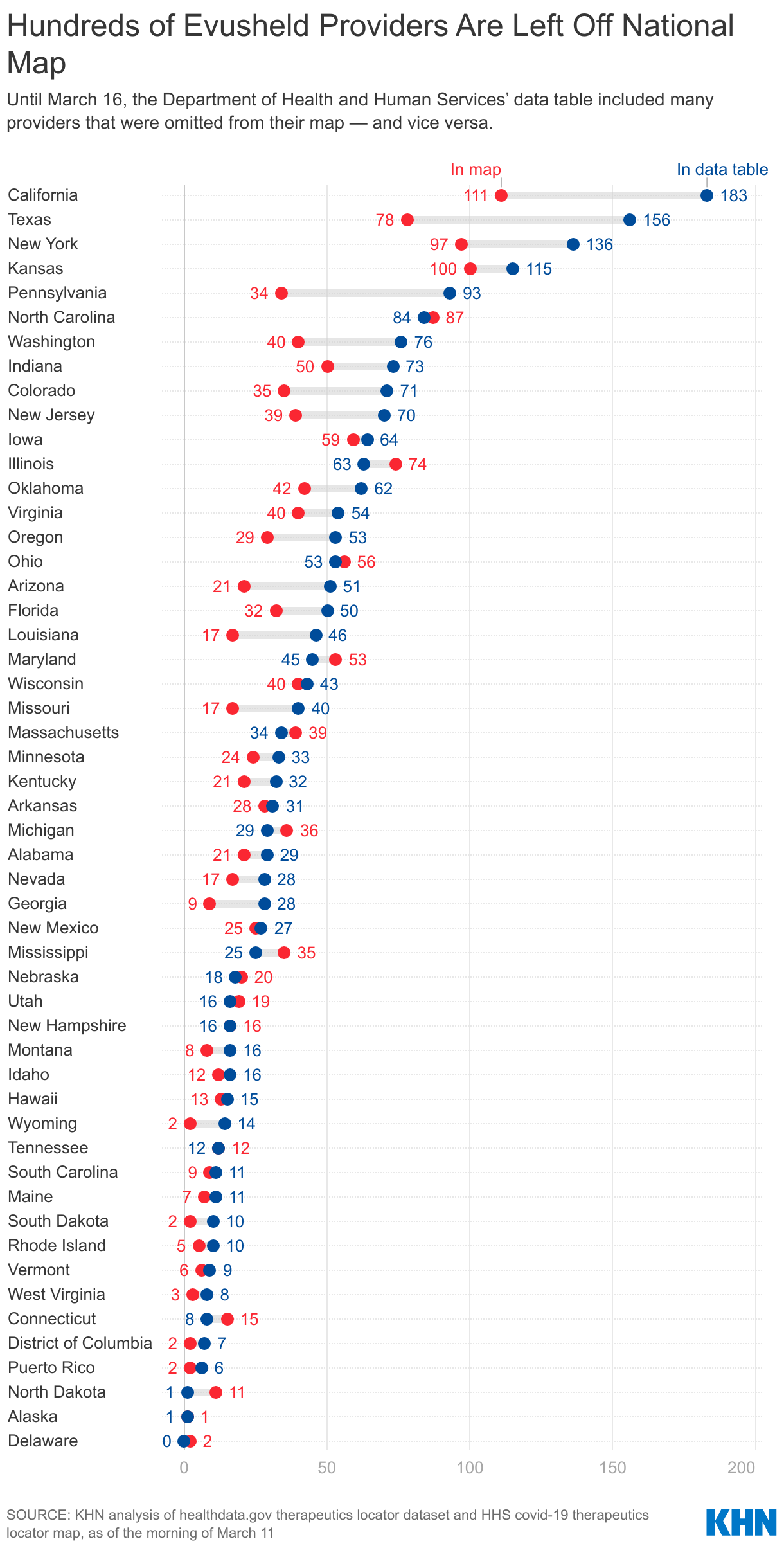
KHN’s analysis of Evusheld provider data published by HHS found that, until March 16, a included several hundred providers that were omitted from the more user-friendly map.
On Wednesday evening, HHS updated the downloadable data file for the first time in eight days, removing hundreds of providers that hadn’t reported how many Evusheld doses they had used in the past week. Several data columns were also removed, including the total number of doses that had been delivered to each site and the most recent delivery date. This information was not publicly available elsewhere; now people seeking Evusheld won’t find those providers on any federal website and data analysts cannot track the pace at which the therapy is being used.
KHN had flagged several discrepancies between the map and the data file to HHS as part of an investigation into the Evusheld rollout across the country. The data file is now nearly identical to what is used on the map, albeit with a few days’ lag.
In Mississippi, for example, 35 Evusheld providers were shown on the map on March 11. Only half of those were also included in the data file. And the data file included yet more providers that weren’t shown on the map.
 ∫⁄¡œ≥‘πœÕ¯ News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF‚Äîan independent source of health policy research, polling, and journalism. Learn more about .
∫⁄¡œ≥‘πœÕ¯ News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF‚Äîan independent source of health policy research, polling, and journalism. Learn more about .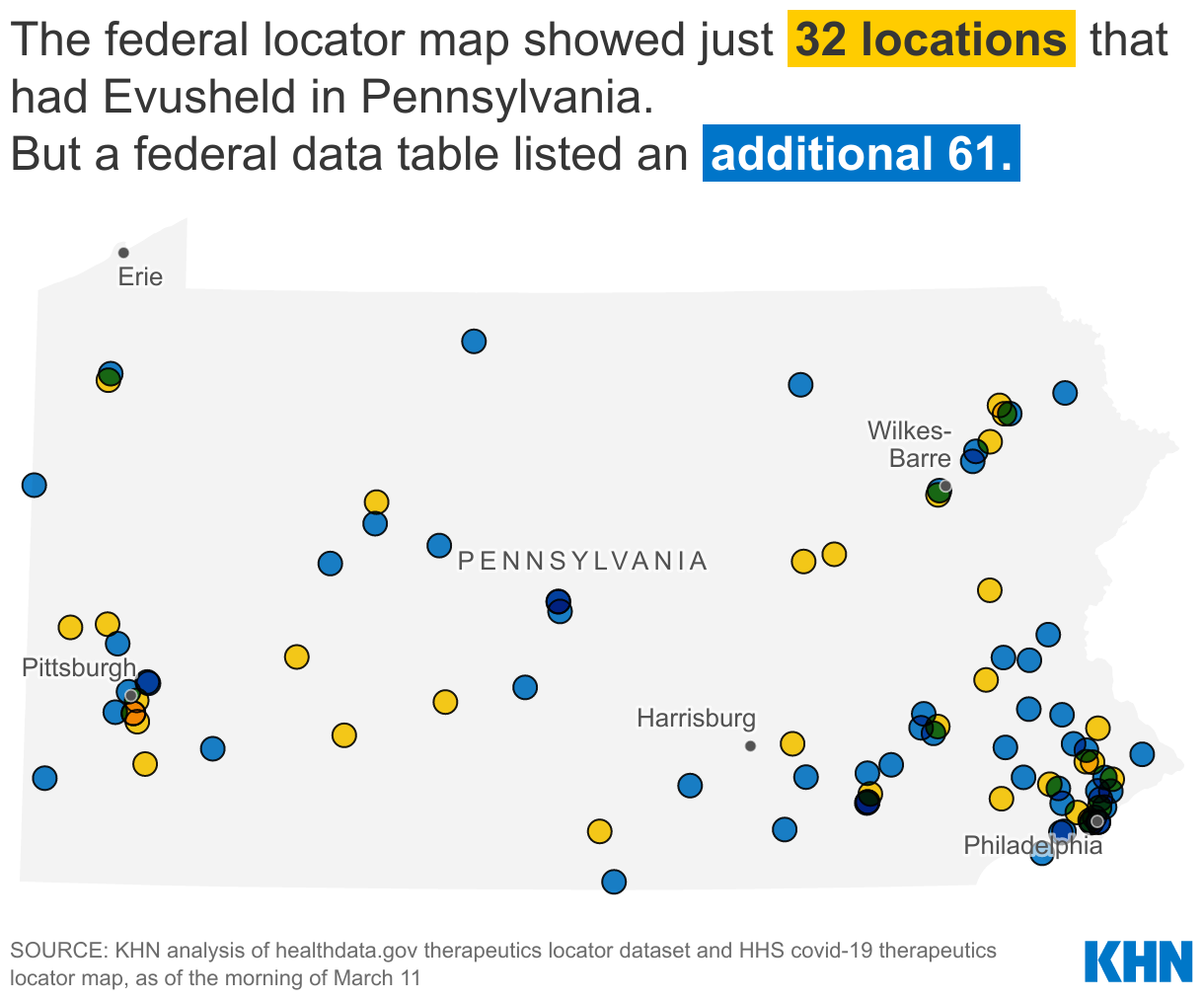
{kind=link}
This <a target="_blank" href="/public-health/evusheld-covid-prevention-monoclonal-antibody-therapy-availability-hhs/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
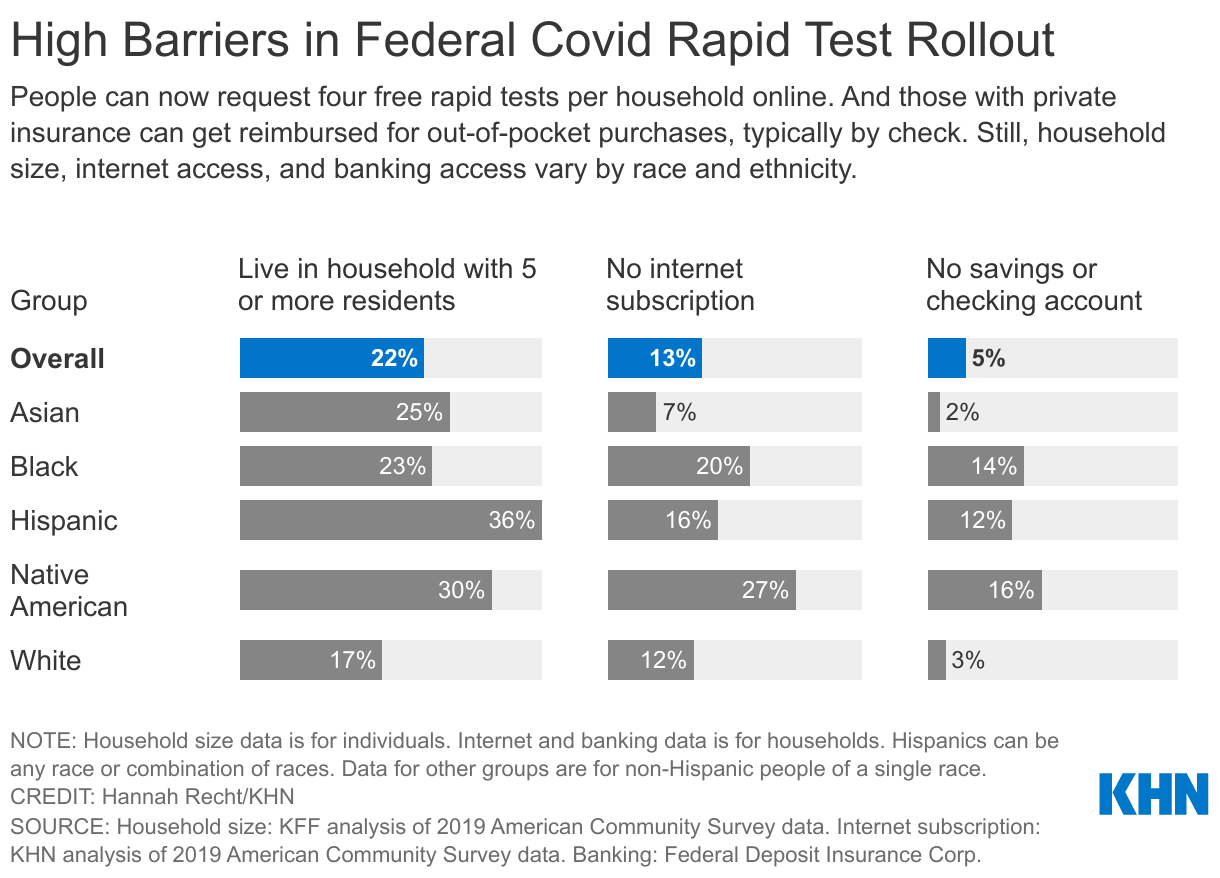
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1464384&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>From the limit placed on test orders to the languages available on websites, the programs stand to leave out many people who don’t speak English or don’t have internet access, as well as those who live in multifamily households. All these barriers are more common for non-white Americans, who have also been by covid. The White House told KHN it will address these problems but did not give specifics.
It launched a on Jan. 18 where people can order free tests sent directly to their homes. But there is a four-test limit per household. Many homes could quickly exceed their allotments — more than a third of Hispanic Americans plus about a quarter of Asian and Black Americans live in households with at least five residents, according to an analysis of Census Bureau data by KFF. Only 17% of white Americans live in these larger groups.
“There are challenges that they have to work on for sure,” said , executive director of the American Public Health Association.
Also, as of Jan. 15, the federal government requires private insurers to reimburse consumers who purchase rapid tests.
When the federal website — with orders fulfilled and shipped through the United States Postal Service — went live this week, the first wave of sign-ups exposed serious issues.
Some people who live in multifamily residences, such as condos, dorms, and houses sectioned off into apartments, reported on social media that if one resident had already ordered tests to their address, the website didn’t allow for a second person to place an order.
“They’re going to have to figure out how to resolve it when you have multiple families living in the same dwelling and each member of the family needs at least one test. I don’t know the answer to that yet,” Benjamin said.
USPS spokesperson David Partenheimer said that while this seems to be a problem for only a small share of orders, people who encounter the issue should file a or contact the help desk at 1-800-ASK-USPS.
A White House official said 20% of shipments will be directed every day to people who live in vulnerable ZIP codes, as determined by the Centers for Disease Control and Prevention’s , which identifies communities most in need of resources.
Another potential obstacle: Currently, only those with access to the internet can order the free rapid tests directly to their homes. Although some people can access the website on smartphones, the online-only access could still exclude millions of Americans: 27% of Native American households and 20% of Black households don’t have an internet subscription, according to a KHN analysis of Census Bureau data.
The federal website is currently available only in English, Spanish, and Chinese.
According to the White House, a phone line is also being launched to ease these types of issues. An aide said it is expected to be up and running by Jan. 21. But details are pending about the hours it will operate and whether translators will be available for people who don’t speak English.
However, the website is reaching one group left behind in the initial vaccine rollout: blind and low-vision Americans who use screen-reading technology. Jared Smith, associate director of WebAIM, a nonprofit web accessibility organization, said the federal site “is very accessible. I see only a very few minor nitpicky things I might tweak.”
The Biden administration emphasized that people have options beyond the rapid-testing website. There are free federal testing locations, for instance, as well as testing capacity at homeless shelters and other congregate settings.
Many Americans with private health plans could get help with the cost of tests from the Biden administration reimbursement directive. In the days since its unveiling, insurers said they have moved quickly to implement the federal requirements. But the new systems have proved difficult to navigate.

Consumers can obtain rapid tests — up to eight a month are covered — at retail stores and pharmacies. If the store is part of their health plan’s rapid-test network, the test is free. If not, they can buy it and seek reimbursement.
The program does not cover the 61 million beneficiaries who get health care through Medicare, or the estimated 31 million people who are uninsured. Medicaid and the Children’s Health Insurance Program are required to cover at-home rapid tests, but rules for those programs vary by state.
And the steps involved are complicated.
First, consumers must figure out which retailers are partnering with their health plans and then pick up the tests at the pharmacy counter. As of Jan. 19, however, only a few insurance companies had set up that direct-purchase option — and nearly all the major participating pharmacies were sold out of eligible rapid tests.
Instead, Americans are left to track down and buy rapid tests on their own and then send receipts to their insurance providers.
Many of the country’s largest insurance companies provide paper forms that customers must print, fill out, and mail along with a receipt and copy of the box’s product code. Only a few, including UnitedHealthcare and Anthem, have online submission options. Highmark, one of the largest Blue Cross and Blue Shield affiliates, for instance, has for its online submission process that involves printing out a PDF form, signing it, and scanning and uploading it to its portal.
Nearly 1 in 4 households don’t own a desktop or laptop computer, according to the Half of U.S. households where no adults speak English don’t have computers.
A KHN reporter checked the websites of several top private insurers and didn’t find information from any of them on alternatives for customers who don’t have computers, don’t speak English, or are unable to access the forms due to disabilities.
UnitedHealthcare and CareFirst spokespeople said that members can call their customer service lines for help with translation or submitting receipts. Several other major insurance companies did not respond to questions.
Once people make it through the submission process, the waiting begins. A month or more after a claim is processed, most insurers send a check in the mail covering the costs.
And that leads to another wrinkle. Not everyone can easily deposit a check. About 1 in 7 Black and 1 in 8 Hispanic households don’t have checking or savings accounts, compared with 1 in 40 white households, according to a . Disabled Americans are also especially likely to be “unbanked.” They would have to pay high fees at check-cashing shops to claim their money.
“It’s critically important that we are getting testing out, but there are limitations with this program,” said , an assistant professor of medicine at the University of Pittsburgh School of Medicine. “These challenges around getting tests to individuals with language barriers or who are homeless are sadly the same drivers of disparities that we see with other health conditions.”
KHN Midwest correspondent Lauren Weber contributed to this report.
∫⁄¡œ≥‘πœÕ¯ News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF‚Äîan independent source of health policy research, polling, and journalism. Learn more about .This <a target="_blank" href="/public-health/biden-administrations-rapid-test-rollout-doesnt-easily-reach-those-who-need-it-most/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
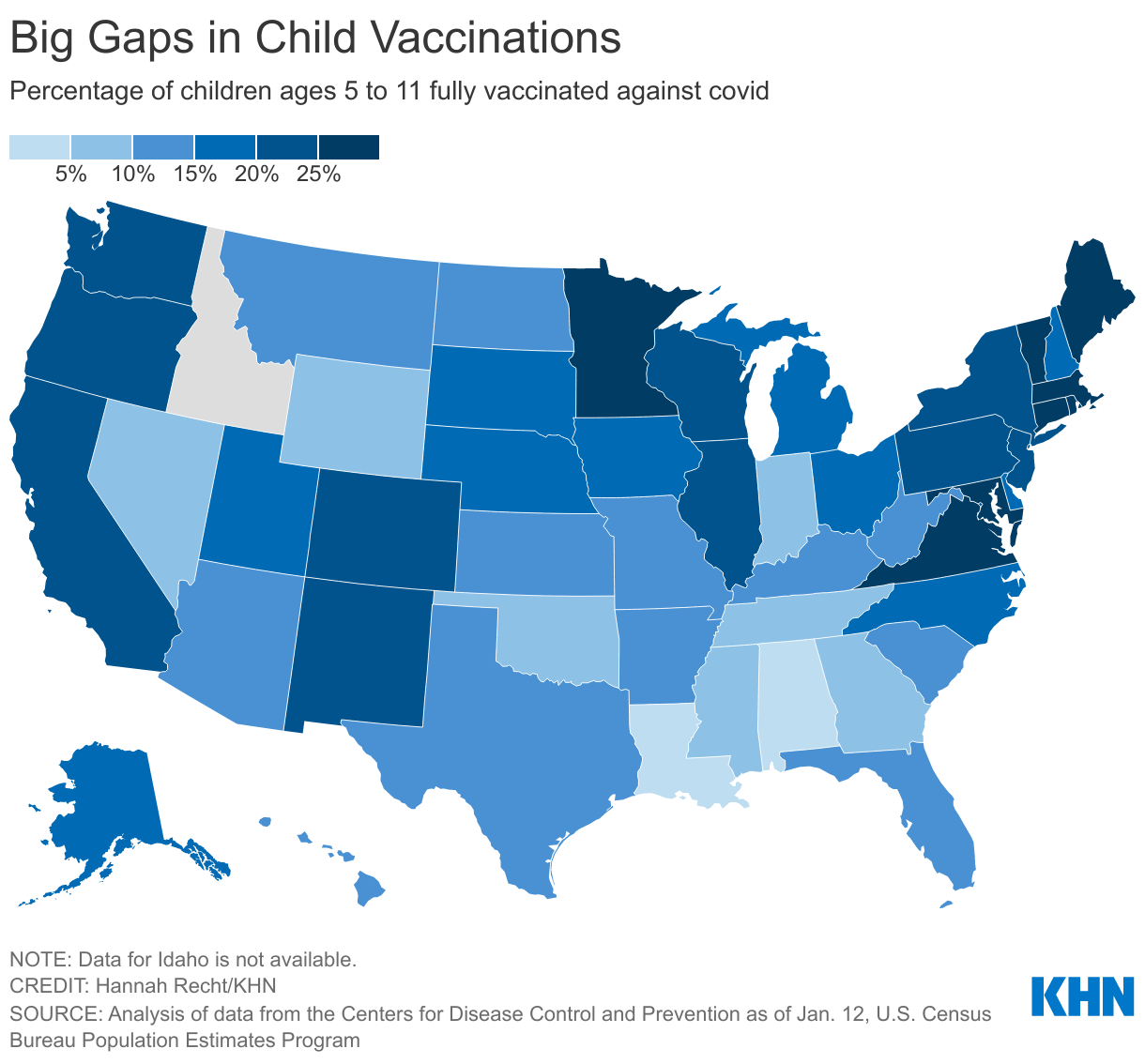
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1434921&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>The national effort to vaccinate children has stalled even as the omicron variant upends schooling for millions of children and their families amid staffing shortages, shutdowns and heated battles over how to safely operate. Vaccination rates vary substantially across the country, a KHN analysis of the federal data shows. Nearly half of Vermont’s 5- to 11-year-olds are fully vaccinated, while fewer than 10% have gotten both shots in nine mostly Southern states.
Pediatricians say the slow pace and geographic disparities are alarming, especially against the backdrop of record numbers of cases and pediatric hospitalizations. School-based vaccine mandates for students, which some pediatricians say are needed to boost rates substantially, remain virtually nonexistent.
“You have these large swaths of vulnerable children who are going to school,” said Dr. Samir Shah, a director at Cincinnati Children’s Hospital Medical Center. Compounding the problem is that states with low vaccination rates “are less likely to require masking or distancing or other nonpartisan public health precautions,” he said.
In Louisiana, where 5% of kids ages 5 to 11 have been fully vaccinated, Gov. John Bel Edwards, a Democrat, added the shot to the list of required school immunizations for the fall, over the objections of state legislators, who are mostly Republicans. The District of Columbia and California, where about 1 in 5 elementary school kids are fully vaccinated, have added similar requirements. But those places are exceptions — 15 states have banned covid vaccine mandates in K-12 schools, according to the .
Mandates are one of multiple “scientifically valid public health strategies,” Shah said. “I do think that what would be ideal; I don’t think that we as a society have a will to do that.”
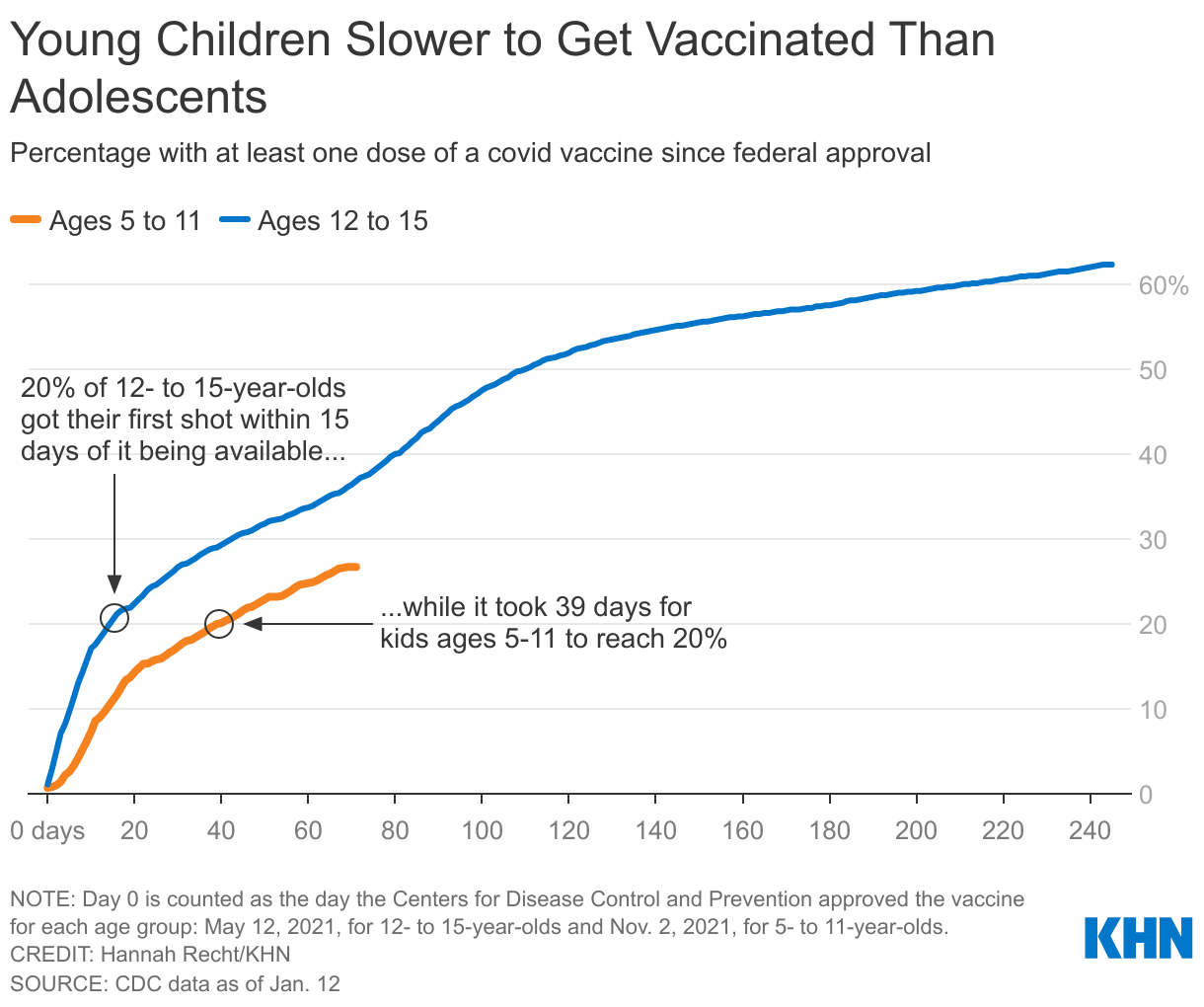
Vaccine demand surged in November, with an initial wave of enthusiasm after the shot was approved for younger children. But parents have vaccinated younger kids at a slower pace than 12- to 15-year-olds, who became eligible in May. It took nearly six weeks for 1 in 5 younger kids to get their first shot, while adolescents reached that milestone in two weeks.
Experts cite several factors slowing the effort: Because kids are less likely than adults to be hospitalized or die from the virus, some parents are less inclined to vaccinate their children. Misinformation campaigns have fueled concerns about immediate and long-term health risks of the vaccine. And finding appointments at pharmacies or with pediatricians has been a bear.
“One of the problems we’ve had is this perception that kids aren’t at risk for serious illness from this virus,” said Dr. Yvonne Maldonado, chair of the American Academy of Pediatrics Committee on Infectious Diseases. “That’s obviously not true.”
Parents are left to weigh which is more of a threat to their children: the covid virus or the vaccine to prevent the virus. Overwhelmingly, research shows, the virus itself presents a greater danger.
Kids can develop debilitating long-covid symptoms or a potentially fatal post-covid . And from the CDC found that children are at significantly higher risk of developing diabetes in the months after a covid infection. Other respiratory infections, like the flu, don’t carry similar risks.
Katharine Lehmann said she had concerns about myocarditis — a rare but serious side effect that causes inflammation of the heart muscle and is more likely to occur in boys than girls — and considered not vaccinating her two sons because of that risk. But after reading up on the side effects, she realized the condition is more likely to occur from the virus than the vaccine. “I felt safe giving it to my kids,” said Lehmann, a physical therapist in Missouri, where 20% of younger kids have gotten at least one dose.
from scientific advisers to the CDC found that myocarditis was extremely rare among vaccinated 5- to 11-year-olds, identifying 12 reported cases as of Dec. 19 out of 8.7 million administered doses.
The huge variations in where children are getting vaccinated reflect what has occurred with other age groups: Children have been much less likely to get shots in the Deep South, where hesitancy, political views and misinformation have blunted adult vaccination rates as well. Alabama has the lowest vaccination rate for 5- to 11-year-olds, with 5% fully vaccinated. States with high adult vaccine rates such as Vermont, Massachusetts, Connecticut and Maine have inoculated the greatest shares of their children.
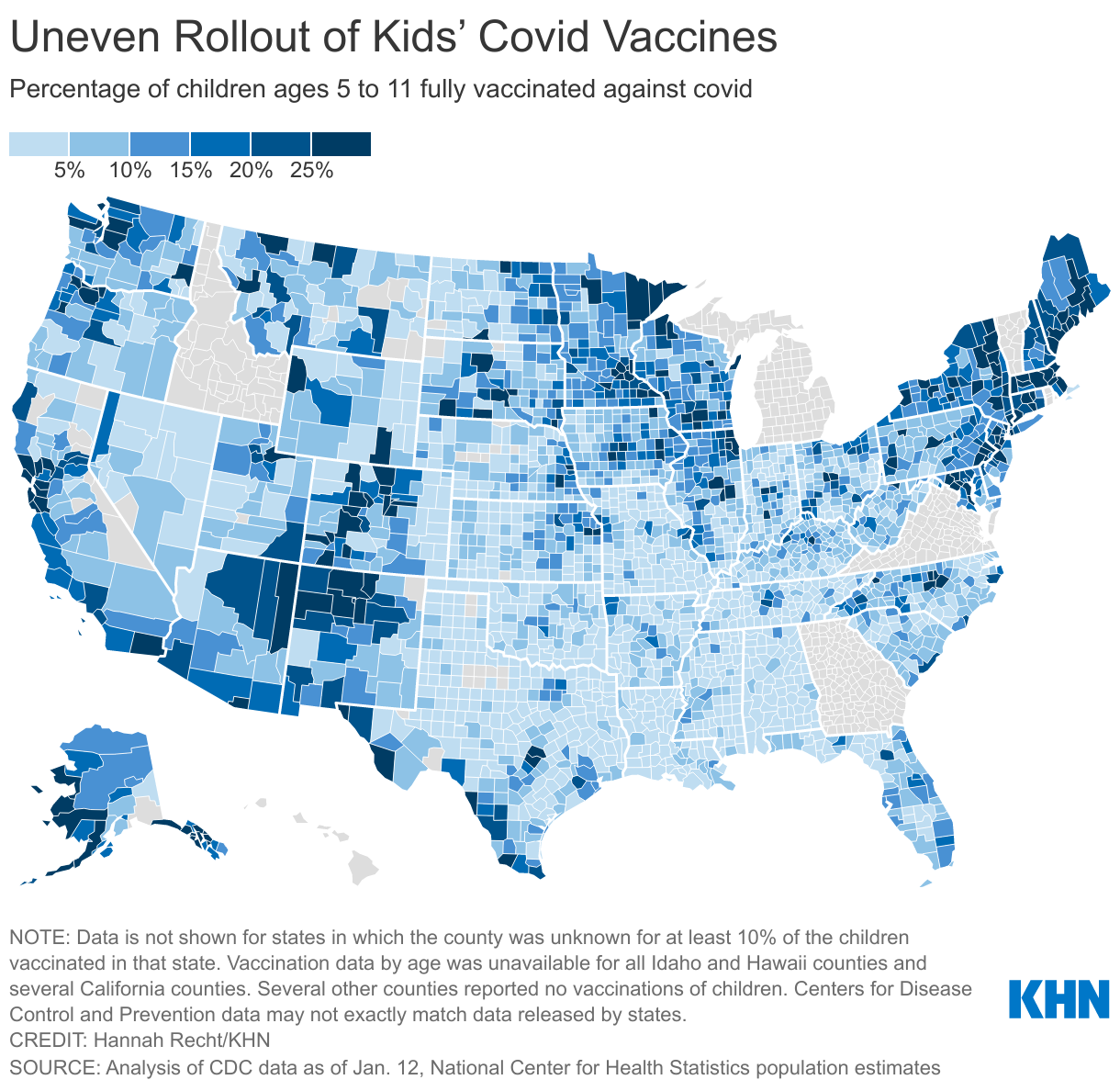
Even within states, rates vary dramatically by county based on political leanings, density and access to the shot. More than a quarter of kids in Illinois’ populous counties around Chicago and Urbana are fully vaccinated, with rates as high as 38% in DuPage County. But rates are still below 10% in many of the state’s rural and Republican-leaning counties. In Maryland, where 1 in 4 kids are fully vaccinated, rates range from more than 40% in Howard and Montgomery counties, wealthy suburban counties, to fewer than 10% along parts of the more rural Eastern Shore.
Nationally, a November found that 29% of parents of 5- to 11-year-olds definitely won’t vaccinate their children and that an additional 7% would do so only if required. Though rates were similar for Black, white and Hispanic parents, political differences and location divided families. Only 22% of wouldn’t vaccinate their kids, while 49% of rural parents were opposed. Half of Republican parents said they definitely wouldn’t vaccinate their kids, compared with just 7% of Democrats.
The White House said officials continue to work with trusted groups to build vaccine confidence and ensure access to shots. “As we’ve seen with adult vaccinations, we expect confidence to grow and more and more kids to be vaccinated across time,” spokesperson Kevin Munoz said in a statement.
The Hunt for Shots
Just before her younger son’s 5th birthday, Lehmann was eager to book covid vaccine appointments for her two boys. But their pediatrician wasn’t offering them. Attempts to book time slots at CVS and Walgreens before her son turned 5 were unsuccessful, even if the appointment occurred after his late-November birthday.
“It was not easy,” she said. Wanting to avoid separate trips for her 10-year-old and 5-year-old, she nabbed appointments at a hospital a half-hour away.
“Both of my kids have gotten all their vaccines at the pediatrician, so I was kind of shocked. That would have certainly been easier,” Lehmann said. “And the kids know those nurses and doctors, so I think it would have helped to not have a stranger doing it.”
The Biden administration has pointed parents to retail pharmacies and 122 children’s hospitals with vaccine clinics. Nationwide, more than 35,000 sites, including pediatricians, federally qualified health centers and children’s hospitals have been set up to vaccinate young kids, according to the administration. Yet administering the covid vaccine to children presents obstacles that haven’t been as prominent for other inoculations.
Enrolling pediatricians in the covid-19 vaccine program is a challenge because of the application process, reporting requirements for administered doses, and staffing, said Claire Hannan, executive director of the Association of Immunization Managers.
“Many of them are short-staffed right now and don’t necessarily have huge capacity to serve,” she said. Plus, “it’s not as easy to engage the schools in school-based clinics in certain areas just due to the political environment.” Health centers, government officials and other groups have set up more than 9,000 school vaccination sites for 5- to 11-year-olds nationwide.
The CDC’s long-standing program, Vaccines for Children, provides free shots for influenza, measles, chickenpox and polio, among others. Roughly are enrolled in the program, which is designed to immunize children who are eligible for Medicaid, are uninsured or underinsured, or are from Native or Indigenous communities. More than half of the program’s providers offer covid shots, although the rates vary by state.
Pharmacies have been heavily used in Illinois, where 25% of 5- to 11-year-olds are fully vaccinated.
Dr. Ngozi Ezike, a pediatrician and the director of the Illinois Department of Public Health, said 53% of shots administered to younger children as of Jan. 5 were done at pharmacies. Twenty percent occurred at private clinics, 7% at local health departments, 6% at federally qualified health centers and 5% at hospitals.
“You need all pieces of the pie” to get more kids vaccinated, Ezike said.
Kids Respond to ‘the Greater Good’
The Levite Jewish Community Center in Birmingham, Alabama, tried to boost vaccinations with a party, offering games and treats, even a photo booth and a DJ, along with shots given by a well-known local pharmacy. Brooke Bowles, the center’s director of marketing and fund development, estimated that about half a dozen of the 42 people who got a dose that mid-December day were kids.
Bowles was struck that children were more likely to roll up their sleeves when their parents emphasized the greater good in getting vaccinated. “Those children were just fantastic,” she said. In parts of the Deep South like this one, pro-vaccine groups face a tough climb — as of Jan. 12, only 7% of Jefferson County’s children had gotten both shots.
The greater good is what pediatricians have emphasized to parents who are on the fence.
“Children are vectors for infectious disease,” said Dr. Eileen Costello, chief of ambulatory pediatrics at Boston Medical Center. “They’re extremely generous with their microbes,” spreading infections to vulnerable relatives and community members who may be more likely to end up in the hospital.
Seventy-eight percent of the hospital’s adult patients have received at least one dose. For children 5 and up, the figure is 39%, with younger children having lower rates than adolescents, Costello said. Particularly amid an onslaught of misinformation, “it has been exhausting to have these long conversations with families who are so hesitant and reluctant,” she said.
Still, she can point to successes: A mother who lost a grandparent to covid was nonetheless reluctant to vaccinate her son with obesity and asthma whom Costello was seeing for a physical. The mother ultimately vaccinated all four of her children after Costello told her that her son’s weight put him at higher risk for severe illness.
“That felt like a triumph to me,” Costello said. “I think her thinking was, ‘Well, he’s a kid — he’s going to be fine.’ And I said, ‘Well, he might be fine, but he might not.’”
Methodology
Vaccination numbers are from the Centers for Disease Control and Prevention as of Jan. 12.
are calculated by the CDC and include vaccinations provided by federal programs such as the Indian Health Service and the Department of Defense, as well as U.S. territories. To compare the vaccination rollout for kids and adolescents, we counted day 0 as the day the CDC approved the vaccine for each age group: , 2021, for 12- to 15-year-olds and , 2021, for 5- to 11-year-olds.
The CDC provides vaccination numbers at the and level. These numbers do not include the small fraction of children who were vaccinated by federal programs. To calculate rates for 5- to 11-year-olds, we divided by the total number of kids ages 5 to 11 in each state or county.
To calculate the number of children ages 5 to 11 in each state, we used the U.S. Census Bureau’s 2019 “single year of age” dataset, the latest release available. For county-level data, we used the National Center for Health Statistics’ , which contain single-year-of-age county-level estimates. We selected the 2019 estimates from the 2020 vintage release so the data would reflect the same year as the state-level estimates.
Vaccination data by age is unavailable for Idaho, counties in Hawaii and several California counties. For county-level vaccination data, we excluded states in which the county was unknown for at least 10% of the kids vaccinated in that state.
Visit the to read more about and download the data.
This <a target="_blank" href="/public-health/as-omicron-surges-effort-to-vaccinate-young-children-stalls/">article</a> first appeared on <a target="_blank" href="">KFF Health News</a> and is republished here under a <a target="_blank" href=" Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=1431814&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>