

OSKALOOSA, Iowa — Rural regions like the one surrounding this southern Iowa town used to have a lot more babies, and many more places to give birth to them.
At least 41 Iowa hospitals their labor and delivery units since 2000. Those facilities, representing about a third of all Iowa hospitals, are located mostly in rural areas where birth numbers have plummeted. In some Iowa counties, annual numbers of births have fallen by three-quarters since the height of the baby boom in the 1950s and ’60s, when many rural hospitals were built or expanded, state and federal records show.
Similar trends are playing out nationwide, as hospitals struggle to maintain staff and facilities to safely handle dwindling numbers of births. of rural U.S. hospitals now lack the service.
“People just aren’t having as many kids,” said Addie Comegys, who lives in southern Iowa and has regularly traveled 45 minutes each way for prenatal checkups at Oskaloosa’s hospital this summer. Her mother had six children, starting in the 1980s, when big families didn’t seem so rare.
“Now, if you have three kids, people are like, ‘Oh my gosh, are you ever going to stop?’” said Comegys, 29, who is expecting her second child in late August.
These days, many Americans choose to have small families or no children at all. Modern birth control methods help make such decisions stick. The trend is amplified in small towns when young adults move away, taking any childbearing potential with them.
Hospital leaders who close obstetrics units often cite declining birth numbers, along with staffing challenges and financial losses. The closures can be a particular challenge for pregnant women who lack the reliable transportation and flexible schedules needed to travel long distances for prenatal care and birthing services.

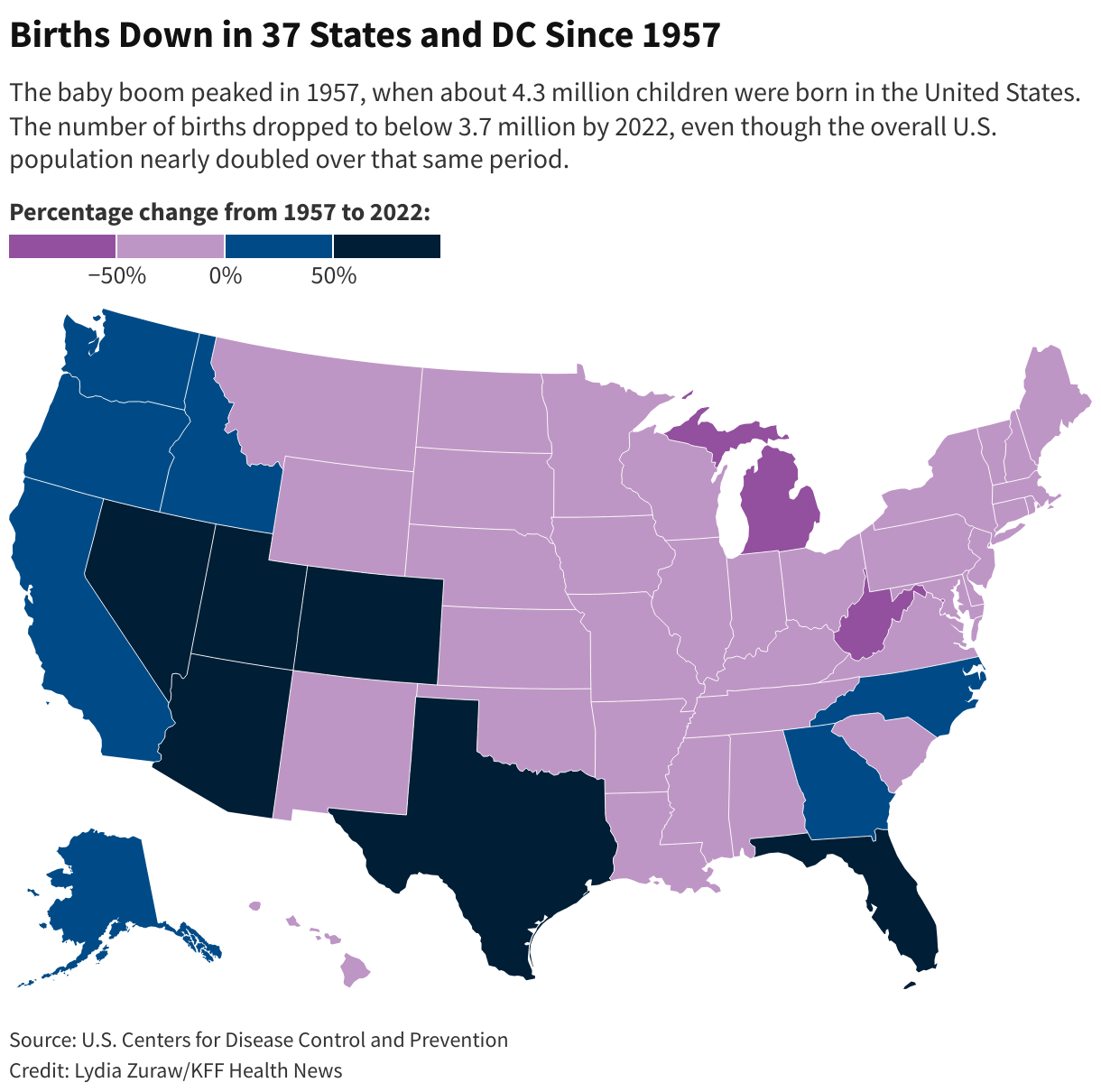
The baby boom peaked in 1957, when about 4.3 million children were born in the United States. The annual number of births dropped below 3.7 million by 2022, even though the overall U.S. population nearly doubled over that same period.
West Virginia has seen the steepest decline in births, a 62% drop in those 65 years, according to federal data. Iowa’s births dropped 43% over that period. Of the state’s 99 counties, just four — all urban or suburban — recorded more births.
Births have increased in only 13 states since 1957. Most of them, such as Arizona, California, Florida, and Nevada, are places that have attracted waves of newcomers from other states and countries. But even those states have had obstetrics units close in rural areas.
In Iowa, Oskaloosa’s hospital has bucked the trend and kept its labor and delivery unit open, partly by pulling in patients from 14 other counties. Last year, the hospital even managed the rare feat of recruiting two obstetrician-gynecologists to expand its services.
The publicly owned hospital, called Mahaska Health, expects to deliver 250 babies this year, up from about 160 in previous years, CEO Kevin DeRonde said.
“It’s an essential service, and we needed to keep it going and grow it,” DeRonde said.


Many of the U.S. hospitals that are now dropping obstetrics units were built or expanded in the mid-1900s, when America went on a rural-hospital building spree, thanks to federal funding from the Hill-Burton Act.
“It was an amazing program,” said , chief operations officer for the National Rural Health Association. “Basically, if you were a county that wanted a hospital, they gave you the money.”
Slabach said that in addition to declining birth numbers, obstetrics units are experiencing a drop in occupancy because most patients go home after a night or two. In the past, patients typically spent several days in the hospital after giving birth.
Dwindling caseloads can raise safety concerns for obstetrics units.
A study in 2023 found that women were more likely to suffer serious complications if they gave birth in rural hospitals that handled 110 or fewer births a year. The authors said they didn’t support closing low-volume units, because that could lead more women to have complications related to traveling for care. Instead, they recommended improving training and coordination among rural health providers.
, a University of Iowa obstetrics and gynecology professor who studies access to birthing services, said it is almost inevitable that when rural birth numbers plunge, some obstetrics units will close. “We talk about that as a bad event, but we don’t really talk about why it happens,” she said.
Radke said maintaining a set number of obstetrics units is less important than ensuring good care for pregnant women and their babies. It’s difficult to maintain quality of care when the staff doesn’t consistently practice deliveries, she said, but it is hard to define that line. “What is realistic?” she said. “I don’t think a unit should be open that only delivers 50 babies a year.”
In some cases, she said, hospitals near each other have consolidated obstetrics units, pooling their resources into one program that has enough staffers and handles sufficient cases. “You’re not always really creating a care desert when that happens,” she said.

The decline in births in recent years. , a sociology professor and demographer at the University of New Hampshire, said it is understandable that many rural hospitals have closed obstetrics units. “I’m actually surprised some of them have lasted as long as they have,” he said.
Johnson said rural areas that have seen the steepest population declines tend to be far from cities and lack recreational attractions, such as mountains or large bodies of water. Some have avoided population losses by attracting immigrant workers, who tend to have larger families in the first generation or two after they move to the U.S., he said.
, a University of Minnesota health policy professor who studies rural issues, said declining birth numbers and obstetric unit closures can create a vicious cycle. Fewer babies being born in a region can lead a birthing unit to shutter. Then the loss of such a unit can discourage young people from moving to the area, driving birth numbers even lower.
In many regions, people with private insurance, flexible schedules, and reliable transportation choose to travel to larger hospitals for their prenatal care and to give birth, Kozhimannil said. That leaves rural hospitals with a larger proportion of patients on Medicaid, a public program that pays about half what private insurance pays for the same services, she said.
Iowa ranks near the bottom of all states for obstetrician-gynecologists per capita. But Oskaloosa’s hospital hit the jackpot last year, when it recruited and , a married couple who both recently finished their obstetrics training. Swartz grew up in the area, and she wanted to return to serve women there.
She hopes the number of obstetrics units will level off after the wave of closures. “It’s not even just for delivery, but we need access just to women’s health care in general,” she said. “I would love to see women’s health care be at the forefront of our government’s mind.”
Swartz noted that the state has only one obstetrics training program, which is at the University of Iowa. She said she and her husband plan to help spark interest in rural obstetrics by hosting University of Iowa residency rotations at the Oskaloosa hospital.
Comegys, a patient of Swartz’s, could have chosen a hospital birthing center closer to her home, but she wasn’t confident in its quality. Other hospitals in her region had shuttered their obstetrics units. She is grateful to have a flexible job, a reliable car, and a supportive family, so she can travel to Oskaloosa for checkups and to give birth there. She knows many other women are not so lucky, and she worries other obstetrics units are at risk.
“It’s sad, but I could see more closing,” she said.